- Volume 60 , Number 1
- Page: 98–100
Long-term follow up of lepromatous leprosy patients receiving intralesional recombinant gamma-lnterferon
To the Editor:
The primary defect in lepromatous leprosy is probably the lack of generation of sensitized T cells (1) which results in deficiency of gamma-interferon (IFN-γ) in the lesion (5). Macrophages in the tissue as well as in the circulation of lepromatous patients remain functionally normal because they release oxygen intermediates when activated by IFN-γ and other antigens (3). Kaplan, et al. in their study on the effect of intralesional recombinant IFN-γ (rIFN-γ) have demonstrated the accumulation of lymphocytes and monocytes, marked thickening of the epidermis, and increased expression of la and γ-IP-10 at the site of injection. With repeated injections of rIFN-γ there was a reduction in OKT-6 cells in the dermis and a distinct fall in the tissue bacterial index (BI) (5,000-10,000-fold) at the site of injection. This was often associated with the formation of an epithelioid granuloma with multinucleated giant cells (2,4). The local changes prompted us to follow these cases to see whether intralesional rIFN-γ also influences tissue response at distant sites.
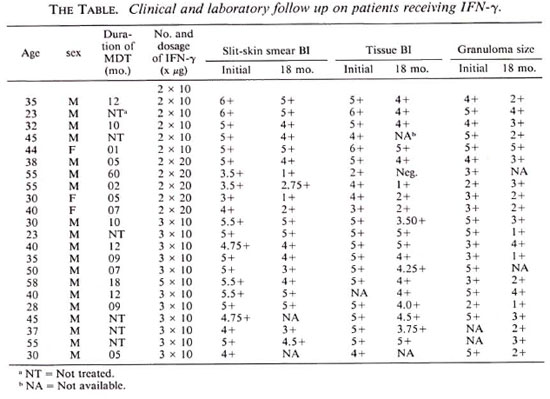
Twenty-two lepromatous leprosy patients (15 LLp, 7 LLs) were included in this study. There were 18 males and four females whose ages ranged from 23-58 years. Out of these 22 patients, six cases were untreated and 15 cases were on treatment for less than 1 year. Only one patient was on antileprosy drugs for more than 5 years. Lyophilized rIFN-γ (Boehringer, Ingelheim am Rhein, Germany) specific activity 2 x 107 U/mg protein was diluted and 10 µ g IFN-γ in 100 µ l of excipient was injected at the lesional site. The number of such injections in an individual patient varied from 1 to 3 or more. If a patient received more than one injection, it was on consecutive days and into the same lesion.
Patients were subjected to clinical charting, slit-skin smear, skin biopsy, and lepromin testing initially and then at an interval of 3-6 months for 18 months. All patients were on conventional multidrug therapy (MDT) throughout the study.
The clinical response in all 22 patients was similar to what we observe with conventional MDT in our clinic. None showed evidence of clinical or histological upgrading or lepromin conversion. Severe erythema nodosum leprosum (ENL) was observed in four patients and mild-to-moderate ENL was seen in seven patients. In two patients neural pain was aggravated.
The average fall in the BI was of 1.0 (Ridley's scale) after 18 months of follow up. Histological examination revealed that the reduction in the size of the granuloma was 1.16 and the fall in the granuloma BI was 1.01 after 18 months of follow up (The Table).
The nature of the infiltrate was predominantly of the macrophage type, and the influx of lymphocytes was insignificant up to 1 year. A noticeable increase in lymphocytes was observed in the biopsies of 18 months' follow up. It was conspicuous that lymphocytic influx was seen more in LLs than in LLp patients. The number of injections of IFN-γ also had no influence on the above parameters.
From this study it can be inferred that in spite of bacterial killing at the site of the rIFN-γ injection by the host macrophages (release of antigenic components) in the presence of large quantities of la molecules and T4 cells, the process of primary sensitization could not be initiated. This suggests that in the LL form ofthe disease there must be some very effective, specific suppressive mechanism or clone deletion which prevents primary sensitization. We are tempted to compare this situation with the studies carried out in the field of contact sensitization, where when an animal was made unresponsive to trinitrophenyl (TNP) by challenging through the intravenous route, the animal remained unresponsive in spite of repeated intradermal injection of TNP (6), We feel that more research is needed for the understanding of the development of specific unresponsiveness and responsiveness in leprosy.
- Narendra K. Mathur, M.D.
Asit Mittal, M.D.
Dinesh Mathur, M.D.
Suresh K. Jain, M.D.
Department of Dermatology
S.M.S. Medical College and Hospital
Jaipur 302004, India
Acknowledgment. The authors wish to acknowledge financial grant no. SP/SO/B-30/87 from the Department of Science and Technology, India, for the support of the work published here. We are grateful to Prof. Z. A. Cohn, Laboratory of Cellular Physiology and Immunology, The Rockefeller University, New York, New York, U.S.A., and Prof. Indira Nath, Department of Biotechnology, All India Institute of Medical Sciences, New Delhi, India, for initiating this project.
REFERENCES
1. GODAL, T. Immunological aspects of leprosypresent status. Prog. Allergy 25 (1978) 211-242.
2. Kaplan, G., Mathur, N. K., Job, C. K., Nath, I. and Cohn, Z. A. Effect of multiple interferon-gamma injections on disposal of Mycobacterium leprae. Proc. Natl. Acad. Sei. U.S.A. 86(1989)8073-8077.
3. Kaplan, G., Nathan, C. F., Gandhi, R., Horwitz, M. A., Levis, W. R. and Cohn, Z. A. Effect of recombinant interferon-γ on hydrogen peroxide-releasing capacity of monocyte-derived macrophages from patients with lepromatous leprosy. J. Immunol. 137(1986)983-987.
4. Kaplan, G., Nusrat, A., Sarno, E. N., Job, C. K., McElrath, J., Porto, J. A., Nathan, C. F. and Cohn, Z. A. Cellular responses to intradermal injection of recombinant human gamma-interferon in lepromatous leprosy patients. Am. J. Pathol. 128(1987)345-353.
5. Nogueira, N., Kaplan, G., Levy, E., Sarno, E. N., Kushner, P., Granelli-Piperno, A., Vieira, L., Colomer-Gould, V., Levis, W., Steinman, R., Yip, Y. K. and Cohn, Z. A. Defective gammainterferon production in leprosy; reversal with antigen and interleukin-2. J. Exp. Med. 158(1983)2165-2170.
6. Ptak, W. and Gershon, R. K. Immunological agnosis: a state that derives from T suppressor cell inhibition of antigen-presenting cells. Proc. Natl. Acad. Sci. U.S.A. 79(1982)2645-2648.
Reprint requests to Dr. N. K. Mathur, C-24 Pecyush Path, Bapu Nagar, Jaipur 302004, India.