- Volume 60 , Number 1
- Page: 8–12
Resolution of type 1 reaction in multibacillary hansen's disease as a result of treatment with cyclosporine
ABSTRACT
Type 1 Hansen's disease reaction (reversal reaction) is believed to result f rom a change in the immune response in patients with borderline Hansen's disease. The only effective therapy for significant type 1 reactions has been systemic corticosteroid therapy. Cyclosporine is an immunosuppressive drug which has been widely used in organ transplantation. We report a case of type 1 reaction complicating borderline leprornatous Hansen's disease. Cyclosporine therapy resulted in prompt and sustained resolution of the reaction. The possible mechanism of action of cyclosporine and the implications regarding the immunopathogenesis of type 1 reaction are discussed.RÉSUMÉ
La réaction de type I de la maladie de Hansen (réaction reverse) est supposée résulter d'une modification dans la réponse immunitaire des patients qui présentent une maladie de Hansen borderline. Le seul traitement efficace pour des réactions de type 1 significatives a été un traitement par corticostéroïdes. La cyclosporine est un médicament immunosuppresseur qui a été largement utilisée pour des transplantations d'organes. Nous rapportons un cas de réaction de type 1 apparaissant comme complication d'une maladie de Hansen de type borderline lépromateux. Un traitement par cyclosporine a permis une rémission prompte et de longue durée de la réaction. Le mécanisme d'action possible de la cyclosporine et les implications en ce qui concerne l'immunopathogénèse de la réaction de type 1 sont discutés.RESUMEN
Se considera que la reacción tipo 1 de la enfermedad de Hansen (reacción reversa) es el resultado de un cambio en la respuesta inmune de los pacientes con enfermedad de Hansen intermedia. Hasta ahora, la única terapia efectiva para el tratamiento de las reacciones de tipo 1. ha sido la administración sistémica de corticoesteroides. La ciclosporina es una droga inmunosupresora que ha sido ampliamente utilizada en los transplantes de órganos. Aquí se reporta un caso de reacción tipo 1 en un paciente con enfermedad de Hansen lepromatosa subpolar cuyo tratamiento con ciclosporina condujo a una rápida y sostenida resolución de la reacción. También se discuten los posibles mecanismos de acción de la ciclosporina y las implicaciones sobre la inmunopatogénesis de la reacción tipo 1.Cyclosporine is a cyclic polypctidc produced by the fungus Tolypocladium inflatum Gams. It is a potent immunosuppressive agent which, since its introduction in 1978 (2), has played a major role in improved results following organ transplantation (3). The only reported use of cyclosporine in Hansen's disease is a 1987 report describing three patients with chronic type 2 reaction (erythema nodosum leprosum) who were treated with the drug (9). We report here what is, to the best of our knowledge, the first case of treatment of type 1 reaction (reversal reaction) with cyclosporine.
CASE REPORT
The patient was a 25-year-old man who came to Hawaii from The Philippines at 15 years of age. There were no signs of Hansen's disease when, because of a strong family history of Hansen's disease, he was examined in 1983 and 1984. He developed a skin eruption in November 1988. This was characterized by multiple 1-2 cm urticarial papules and plaques, primarily on the upper and lower extremities, with a few lesions on the chest and earlobes. There was no sensory loss. There was questionable enlargement of the ulnar nerves but no other neurologic abnormality. Skin biopsy microscopic sections (Figs. 1A and IB) showed changes of borderline leprosy (BL-BB) consisting of a patchy granulomatous infiltrate comprised of histiocytes intermingled with many lymphocytes and plasma cells. The infiltrate involved 30º/o-40% of the dermis. A moderate number of solid-staining acidfast bacilli (AFB) were seen. Slit-skin smears showed a bacterial index (BI) ranging from 2.0 to 4.5 and a morphological index (MI) ranging from 1.0%-3.0%. Mouse foot pad testing of a skin biopsy showed no resistance to dapsone, rifampin, or clofazimine.
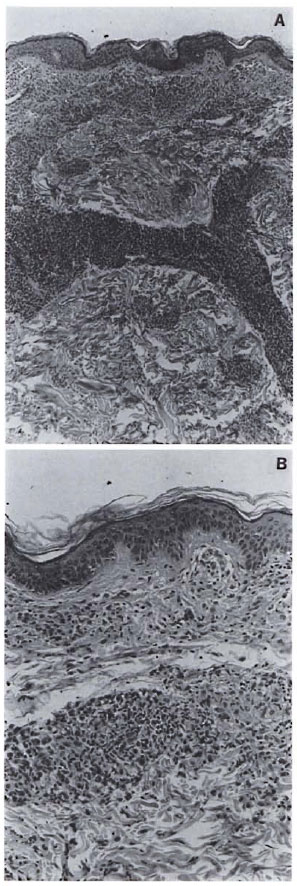
Fig. 1. Photomicrograph of initial skin biopsy, November 1988. A = Granulomatous infiltrate involving 40% of dermis [Hematoxylin and eosin (H&E) x 40]. B = Histiocytes with moderate infiltrate of lymphocytes and plasma cells (H&E x 100).
Treatment with rifampin 600 mg daily and clofazimine 100 mg daily was initiated in November 1988. The primary physician chose not to include dapsone in the regimen because of mild microcytic anemia suggestive of thalassemia and concern about dapsone-induced hemolysis. Rapid improvement was noted, and the dose of clofazimine was reduced to 50 mg daily in January 1989. In April 1989, after approximately 6 months of treatment, increased redness and swelling of the pre-existing skin lesions as well as similar-appearing new skin lesions and enlargement of the right ulnar nerve were noted. The skin lesions were not tender. There were no associated systemic symptoms such as fever, anorexia, or lassitude. In May 1989, skin-biopsy microscopic sections showed changes of borderline leprosy (BL-BB) with reversal reaction consisting of a granulomatous infiltrate involving 75% of the dermis. The infiltrate was comprised of histiocytes with many lymphocytes and plasma cells. The histiocytes showed mild epithelioid cell differentiation in focal areas. A moderate number of AFB were seen, and these were generally fragmented or beaded. Slit-skin smears showed no change in the BI, but the MI had fallen to 1.0%. Corticosteroid therapy was initiated, initially prednisone 20 mg daily. His skin lesions persisted, and he developed edema of the hand. The prednisone was increased to 100 mg daily in May 1989, and the patient improved markedly shortly thereafter. Erythema and edema of the skin lesions recurred intermittently as the prednisone was tapered, though overall there was a good response. After approximately 3 months of prednisone therapy, when the dose had been lowered to 40 mg daily, he developed severe cystic acne, mainly on the face. This did not respond to the usual measures. The patient refused additional prednisone therapy, and he refused any further treatment for about 2 months.
When he was evaluated in October 1989, he had multiple skin nodules as well as a large indurated patch on the left arm and hand. The earlobes were red and indurated. The right ulnar nerve was enlarged and tender. Skin-biopsy microscopic sections (Figs. 2A and 213) showed epithelioid cell granulomas diffusely filling the dermis and extending into the subcutis. The granulomas showed moderate edema, and were surrounded by a dense infiltrate of lymphocytes. Only rare poorly staining bacilli were present. A diagnosis of persistent type 1 reaction was made. He refused to take any more prednisone. With fully informed consent, treatment was initiated with cyclosporine at a dose of 7 mg/kg per day in November 1989. Reduction in the erythema and induration of the skin lesions was apparent within 10 days. The trough serum cyclosporine level was 28 ng/ml. The daily dose was therefore increased in 11 mg/kg. The trough serum cyclosporine level was 50 ng/ml on this dose. Clinically there was progressive improvement in the type 1 reaction. The dose of cyclosporine was increased to 20 mg/kg per day. At this dose, the trough scrum level was 57 ng/ml. Because of the excellent clinical response, the dose was not increased. The patient continued on the same doses of cyclosporine, rifampin, and clofazimine. His type 1 reaction resolved by March 1990. Cyclosporine was discontinued in June 1990 after 8 months of treatment. He has continued on rifampin and clofazimine therapy and has done well. A skin biopsy in December 1990 showed involuting Hansen's disease with no evidence of type 1 reaction. There were no AFB. Slitskin smears from four sites at that time showed no bacilli. The patient has continued to feel well. There has been no recurrence of the type 1 reaction during the 1-year period since the drug was stopped.
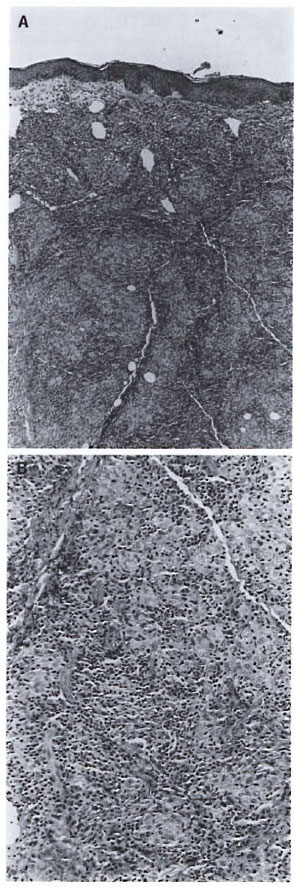
Fig. 2. Photomicrograph of skin biopsy, October 1989, prior to cyclosporine therapy. A = Granulomatous infiltrate involving entire dermis (H&E x 40). B = Epithelioid granulomas with dense infiltrate of lymphocytes (H&E x 100).
The patient was known prior to cyclosporine therapy to be a chronic carrier of the hepatitis B virus. There were no clinical or biochemical changes in his chronic hepatitis B infection prior to the development of the type 1 reaction. There was no change in his liver function during the course of cyclosporine, nor did he experience any other adverse effects. He has had no problems with cystic acne since late 1989.
DISCUSSION
Hansen's disease is characterized by a spectrum of immunity, with many of the features believed to be due to variable resistance to Mycobacterium leprae, the etiologic agent. Thus, individuals with selfhealing, subclinical infection are believed to have a high degree of cell-mediated immunity (CMI) to this organism; those with tuberculoid and borderline disease progressively lower degrees of CMI, and those with polar lepromatous leprosy little or no CMI (13,14)
In addition to this basic role of the immune system, a primary change in the immune response to M. leprae or a change secondary to some other stimulus is believed to play a critical role in the so-called reactional states of Hansen's disease, including type 1 reaction or reversal reaction and type 2 reaction or erythema nosodum leprosum (ENL) (5). While the specific immunopathologic mechanisms of these reactional states have yet to be determined, changes in cells which are critical in CMI have been found in clinical studies of patients with reactions. Thus Modlin, el al. found a reduced percentage of M. leprae antigen-specific CD8+ (suppressor) cells during type 2 reactions followed by restoration of suppres sor cell numbers when the reaction subsided (10). On the other hand, studies of skin biopsies (11) and suction-induced blisters (16) have shown an increased number of CD4+ (T-helper) cells associated with type 1 reactions.
Type 1 reactions are found in individuals with borderline Hansen's disease, while type 2 reactions are confined to those with heavy bacillary loads, i.e., lepromatous or borderline lepromatous disease. Corticosteroids are the primary therapeutic modality for both types of reactions. In type 2 reactions, thalidomide is a very effective alternate agent for those who do not respond to or are intolerant of corticosteroids. There is no satisfactory substitute for corticosteroids in type 1 reactions.
Cyclosporine was approved for use in 1983. It differs from earlier immunosuppressive agents in selectively inhibiting adaptive immune responses. Although the precise mechanism of action is unknown, cyclosporine appears to revcrsibly inhibit helper-T cells while not affecting suppressor-T cells (6). Thus this drug might be expected to be beneficial in type 1 reactions if the increase in helper-T cells referred to above is indeed important in the pathogenesis of this condition.
Blood levels of cyclosporine during oral therapy are quite variable. Therefore, transplant programs monitor serum or plasma levels, with measurements of the trough level preferred (3). Favorable therapeutic outcomes correlate to some degree with trough serum levels between 100 and 250 ng/ml (8), although the pharmacokinetics of cyclosporine are extremely variable and complicated (7). This patient's clinical improvement when the trough level was only 28 ng/ ml, along with his remission of more than 1 year when the maximum trough level attained was 57 ng/ml, suggests that the dose and desirable blood level of cyclosporine may vary with the therapeutic indication.
The only approved uses for cyclosporine are for the prevention of organ rejection and the treatment of chronic rejection in allogenic organ transplantation. This agent also appears to be effective in graft-versus-host disease, psoriasis, and various hematologic, dermatologic, and connective tissue diseases(1,18). The major adverse effects are hypertension and renal dysfunction, the latter clearly dose-related (12).
Because the metabolism of cyclosporine is cytochrome P-450-dependent, it interacts with a number of drugs. Rifampin lowers the serum level of cyclosporine, probably by means of induction of microsomal enzymes (15). This may explain the relatively low serum levels in our patient. Although we were concerned about the use of this drug in a patient who is a chronic carrier of the hepatitis B virus, other studies have shown that most hepatitis B carriers tolerate the drug (4,17)
While cyclosporine was well tolerated in our patient and one might hope that type 1 Hansen's disease reaction will generally respond to a lower dose of cyclosporine than that required for transplantation with a consequent decrease in the incidence of adverse effects, the role of this drug in the treatment of such reactions is clearly limited at this time by the cost of the drug. Even at the low dose used in this patient, the cost of the cyclosporine at 20 mg/kg per day was approximately $83 per day and the total cost for the 8-month course of treatment was approximately $17,750. Nevertheless, the experience with this patient suggests that there is an alternative for those patients with severe type 1 Hansen's disease reaction who cannot tolerate or do not respond to corticosteroid therapy. In addition, this patient's course does support the findings of previous laboratory studies regarding the immunopathology and pathogenesis of type 1 reactions, and suggests that cyclosporine may be useful in elucidating the etiology of these reactions.
REFERENCES
1. BACH, J. F. Cyclosporine in autoimmune diseases. Transplant. Proc. 21 Suppl. 1(1989)97-113.
2. CALNE, R. Y., WHITE, D. J. G., THIRU, S., EVANS, D. B., MCMASTER. P., DUNN. P. C. CRADDOCK. G. N., PENTLOW, D. B. and ROLLES. K. Cyclosporin A in patients receiving renal allografts from cadaver donors. Lancet 21978)1323-1327.
3. DE GROEN. P. C. Clycosporine: a review and its specific use in liver transplantation. Mayo Clin. Proc. 64(1989)680-689.
4. HUANG, C.-C. LAI. M.-K. and FONG .M.-T . Hepatitis B liver disease in cyclosporine-treated renal allograft recipients. Transplantation 49( 1990)540-544.
5. JOPLING, W. H. Leprosy reactions (reactional states). In: Handbook of Leprosy. London: William Heinemann Medical Books, 1971, p. 42.
6. KAHAN, B. D. Cyclosporine. N. Engl. J. Med. 321(1989)1725-1738.
7. KAHAN. B. D. and GREVEL, J. Optimization of cyclosporine therapy in renal transplantation by a pharmacokinetic strategy. Transplantation 46(1988)631-644.
8. KAHAN, B. D., WIDEMAN, C. A., REID, M., GIBBONS, S., JAROWENKO, M., FLECHNER. S. and VAN BUREN, C. T. The value of serial serum trough cyclosporine levels in human renal transplantation. Transplant. Proc. 16(1984)1195-1199.
9. MILLER, R. A., SHEN, J. Y., REA. T. H. and HARNISCH, J. P. Treatment of chronic erythema nodosum leprosum with cyclosporine A produces clinical and immunohistologic remission. Int. J. Lepr. 55(1987)441-449.
10. MODLIN. R. L., MEHRA, V., JORDAN, R., BLOOM, B. R. and REA, T. H, In situ and in vitro characterization of the cellular immune response in erythema nodosum leprosum. J. Immunol. 136(1986)833-886.
11. NARAYANAN, R. B., LAAL, S., SHARMA, A. K., BHUTANI, L. K. and NATH. I. Differences in predominant T cell phenotypes and distribution pattern in reactional lesions of tuberculoid and leprornatous leprosy. Clin. Exp. Immunol. 55(1984)623-628.
12. PORTER, G. A., BENNETT, W. M. and SHEPS. S. G. Cyclosporine-associated hypertension. Arch. Intern. Med. 150(1990)280-283.
13. RIDLEY, D. S. and JOPLING. W. H. Classification of leprosy according to immunity, a five-group system. Int. J. Lepr. 34(1966)255-273.
14. SAMPATAVANICH. S., SAMPOONACHOT, P., KONG-SUEBCHART, K., RAMASOOTA, T., PlNRAT, U., MONGKOLWONGROI. P., OZAWA. T., SASAKI, N. and ABE. M. Immunoepidemiological studies on subclinical infection among leprosy household contacts in Thailand. Int. J. Lepr. 57(1989)752-765.
15. SANDS, M. and BROWN, R. B. Interactions of cyclosporine with antimicrobial agents. Rev. Infect. Dis. 11(1989)691-697.
16. SCOLLARD, D. M., SURIYANON, V., BHOOPAT. L., WAGNER. D. K., SMITH, T. C, THAMPRASERT, K., NELSON, D. L. and THEETRANOT. C. Studies of human leprosy lesions in situ using suction-induced blisters. 2. Cell changes and soluble interleukin 2 receptor (Tac peptide) in reversal reactions. Int. J. Lepr. 58(1990)469-479.
17. STEMPEL. C, LAKE, J., FERRELL, L.,TOMLANOVICH, S., AMEND, W., SALVATIERRA. O. and VINCENTI, F. Effect of cyclosporine on the clinical course of HbsAG-positive renal transplant patients. Transplant. Proc. 23(1991)1251-1252.
18. WILKE, W. S., CAMISA. C. and LICHTIN. A. Novel uses of cyclosporine A. Cleveland Clin. J. Med. 57(1990)116-117.
1. M.D., M.P.H., Chief, Tuberculosis/ Hansen's Disease Control Branch, State of Hawaii Department of Health (present position: Associate Professor of Medicine, University of Hawaii School of Medicine. Honolulu, Hawaii).
2. M.D., Dermatologist, Honolulu. Hawaii.
3. M.D., Department of Dermatology, Straub Clinic and Hospital, Honolulu, Hawaii.
4. M.D., Dermatologist. Honolulu, Hawaii, U.S.A. (present position: Assistant Professor of Medicine (Dermatology). UCLA School of Medicine, Los Angeles. California. U.S.A.).
Reprint requests to Richard I. Frankel, M.D., M.P.H., 1356 Lusitana Street #509, Honolulu, Hawaii 96813, U.S.A.
Received for publication on 19 August 1991.
Accepted for publication on 13 November 1991.