- Volume 60 , Number 1
- Page: 81–2
How effective is monthly rifampin?
This department is for the publication of informal communications that are of interest because they are informative and stimulating, and for the discussion of controversial matters. The mandate of this JORNAL is to disseminate information relating to leprosy in particular and also other mycobacterial diseases. Dissident comment or interpretation on published research is of course valid, but personality attacks on individuals would seem unnecessary. Political comments, valid or not, also are unwelcome. They might result in interference with the distribution of the JOURNAL and thus interfere with its prime purpose.
To the Editor:
The World Health Organization (WHO) Study Group of 1982 (6) believed that ". . . there is no evidence that monthly doses of rifampin are less effective than daily doses." This view has since been refuted by the following evidence.
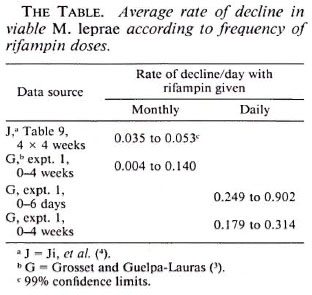
Viable Mycobacterium leprae declined at the average rate shown in The Table (1) during treatment of infected mice with rifampin at 10 mg/kg/day (by gavage). The calculations use standard methods (2) based on ID50s. Viable M. leprae decline at a rate of at least 0.249 per day during daily rifampin treatment but no more than 0.053 per day during treatment with rifampin monthly.
A patient ingesting only the monthly supervised rifampin doses of the WHO multidrug therapy regimen (WHO MDT) is predicted to have, after 14 weeks, at least 100 million times more viable M. leprae than a patient ingesting rifampin daily (The Figure). This vast difference is expected to be missed by skin smears or biopsies, which do not adequately distinguish between viable and nonviable acid-fast M. leprae.
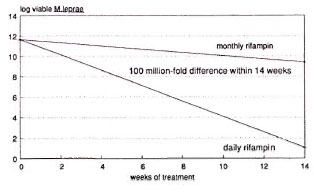
The figure. Predicted decline in viable M. leprae according to frequency of rifampin doses in lepromatous leprosy patients based on measured rate of declineamong viable M. leprae in mouse experiments.
The supervised monthly ingestion of rifampin is, therefore, a relatively ineffective safeguard against the failure of some patients to ingest their prescribed drugs regularly. A monthly injection of dapsone (5) is at present the only method of fully supervised intermittent chemotherapy which does not involve important sacrifice of efficacy against M. leprae.
The role of monthly rifampin in the treatment of leprosy is questionable on biological grounds.
- Joel G. Almeida, M.B.B.S, Ph.D.
P.O. Box 25
Kodaikanal 624101, India
REFERENCES
1. ALMEIDA, J. G. Leprosy: short-term treatment. A quantitative scientific basis for anti-microbial chemotherapy in leprosy control programmes. U.K.: Plateau, 1990, p. 106.
2. FINNEY, D. J. Assays based on quantal responses. In: Statistical Method in Biological Assay. London: Charles Griffin and Co. Ltd., 1978, pp. 394-401.
3. GROSSET, J. H. and GUELPA-LAURAS, C. C. Activity of rifampin in infections of normal mice with M. leprae. Int. J. Lepr. 55 Suppl.(1987)847-851.
4. Ji, B., CHEN, J., LU, X., W ANG, S., NI, G., HON, Y., ZHOU, D. and TANG, Q. Antimycobactcrial activities of two newer ansamycins, R-76-1 and DL 473. Int. J. Lepr. 54(1986)563-577.
5. PIETERS, F. A., WOONINK, F. and ZUIDEMA, J. field trial among leprosy patients in Nigeria with depot injections of dapsone and monoactyldapsone. Int. J. Lepr. 54(1986)383-388.
6. WHO S TUDY G ROUP. Chemotherapy of leprosy for control programmes. Geneva: World Health Organization, 1982, p. 33. Tech. Rep. Ser. 685.