- Volume 59 , Number 1
- Page: 20–4
Serum zinc/copper ratio in subtypes of leprosy and effect of oral zinc therapy on reactional states
ABSTRACT
Serum zinc and copper levels and zinc/ copper ratios were studied in 86 healthy controls, 45 cases of borderline tuberculoid (BT), 31 cases of borderline lepromatous (BL), 117 cases of lepromatous (LL) leprosy patients, 16 cases with severe erythema no dosum leprosum (ENL) reaction, and 16 cases with EN L reaction receiving oral zinc therapy. A significant reduction in serum zinc levels was noticed in all types of leprosy, the maximum decrease being seen in cases with EN L reaction. Conversely, the copper levels were significantly increased from BT to LL cases with EN L reaction in a progressive manner. A very good negative correlation (r = -0.998) was noticed between mean serum zinc and copper levels from healthy controls to active LL cases with EN L reaction. After oral zinc therapy, the serum zinc levels were significantly increased in all of the 16 LL patients with ENL reaction. In contrast, the copper levels were not decreased, indicating that oral zinc therapy can restore normal zinc levels in leprosy patients but is unable to reduce the increased copper levels.RÉSUMÉ
Les taux de zinc et cuivre sériques et les ratios zinc/ cuivre ont été étudiés chez 86 témoins, 45 cas de lèpre borderlinc tuberculoïde (BT), 31 cas de lèpre borderlinc lépromatcuse (BL), 1 17 patients présentant une lèpre lépromatcusc (LL), 16 cas ayant une réaction sévère d'érythème noueux lépreux (ENL) et 16 cas avec un ENL recevant un traitement à base de zinc par voie orale. Une diminution significative des taux de zinc sérique fut notée pour tous les types de lèpre, la diminution maximale étant vue parmi les cas de réaction ENL. Au contraire, les taux de cuivre étaient augmentés de manière signficative et progressivement depuis les cas BT jusqu'aux LL présentant une réaction ENL. Une très bonne corrélation négative (r = -0, 998) fut trouvée entre les taux sériques moyen de zinc et de cuivre depuis les témoins en bonne santé jusqu'aux malades LL actifs avec une réaction ENL. Après traitement au zinc par voie orale, les taux sériques de zinc étaient significativement augmentés chez, tous les 16 patients LL avec une réaction ENL. Par contraste, les taux de cuivre n'étaient pas diminués, indiquant qu'un traitement au zinc par voie orale peut rétablir des taux normaux de zinc chez les malades de la lèpre, mais ne peut faire diminuer les taux augmentés de cuivre.RESUMEN
Se estudiaron los niveles de zinc y cobre, y la relación zinc/cobre, en 86 controles sanos, 45 casos de lepra intcrmcdia-tubcrculoide (BT), 31 casos lepromatosos subpolares (BL), 117 casos lepromatosos (LL), 16 casos con severa reacción tipo eritema nudoso leproso (ENL), y 16 casos con reacción ENL bajo tratamiento con zinc oral. En todos los casos se observó una significante reducción en los niveles séricos de zinc pero ésta fue máxima en los casos con reacción ENL. Por el contrario, los niveles de cobre aumentaron significativa-y progresivamente de los casos BT a los casos LL con reacción ENL. Yendo de los controles sanos a los casos LL activos con reacción ENL, se notó una buena correlación negativa (r = -0.998) entre los niveles medios de zinc y cobre séricos. Después de la terapia con zinc oral, los niveles séricos de zinc estuvieron significativamente elevados en los 16 pacientes LL con reacción ENL pero sus niveles de cobre no estuvieron disminuidos. Esto indica que que la terapia con zinc oral puede restaurar los niveles normales de zinc en los pacientes con lepra pero es incapaz de reducir los niveles de cobre sérico.The role of trace elements such as zinc and copper in a chronic infectious disease, such as leprosy, has been well understood in recent years. Zinc is a vital clement in a number of enzyme systems (5,16,18). In human beings, zinc deficiency results in thymus atrophy (6) and impaired cell-mediated immune (CMI) reactions (1,12,14). Zinc deficiency in various pathological conditions manifested by malnutrition was first observed by Prasad and co-workers (19,20). Significant decreases in serum zinc levels in all types of leprosy, except tuberculoid, have been reported (11,22). A close association between chronic skin ulceration and lowered scrum and skin zinc concentrations has been noticed in leprosy (7,13,23). Copper plays an important role in a number of metallocnzymes, including cytochrome c oxidase, superoxide dismutase, and lysyl oxidase (15,17,25). An increase in serum copper in acute and chronic infections has been reported (2). Ramu and Nagarajan (21) have observed an increased concentration of serum copper in reactional states of lepromatous leprosy. Vcnkatesan, et al. (30) have noticed hypercuprcmia along with lowered serum zinc levels in active lepromatous leprosy and in leprosy patients in reactional states.
In the present study, serum zinc and copper levels and serum zinc/copper ratios were estimated in a large number of subjects who included leprosy patients across the spectrum of the disease, patients with lepra reaction with and without oral zinc therapy, and healthy controls.
MATERIALS AND METHODS
A total of 225 leprosy patients (both outpatients and inpatients) and 86 healthy controls were included in the study. Out of the 225 leprosy patients, 45 were borderline tuberculoid (BT), 31 were borderline lepromatous (BL), and 117 were lepromalous (LL). The remaining subjects of the study were 16 LL cases with erythema nodosum leprosum (ENL) reaction and another 16 cases with ENL reaction receiving oral zinc therapy.
The staff members and trainees of the institutions (Central Leprosy Teaching and Research Institute, Chcngalpattu, and Sacred Heart Leprosy Centre, Kumbakonam, India) served as healthy controls. The patients included in the study were also drawn from both institutions, and only adults in the age group 18-60 were included in the study. The socioeconomic and nutritional status of the patients was not very different from that of the control group. Each of the 16 cases with ENL reaction was given zinc sulfate (ZnS047H20) orally at a daily dose of 225 mg for a period of 6 weeks. They were also given steroids as routine treatment for reaction.
Sample collections. Fasting blood samples were collected from the patients and healthy controls by venipuncture, using zincfree syringes and stainless-steel needles, and the serum was then separated. Hemolyzcd sera and hepatitis cases were not included in the study, and extreme care was taken to avoid zinc contamination. Methods of estimation. Serum zinc and copper levels were estimated by atomic absorption spectrophotometry using an airacetylene flame. A Varian Techtron modelAA-1475 (Varian Instrument Division, Palo Alto, California, U.S.A.) atomic absorption spectrophotometer was used throughout the study.
Estimation of zinc. For measurement, a zinc, hollow cathode lamp was used and the current adjusted to 5 ma. The monochrometer was set at 213.9 nm with a spectral band pass (slit width) of 1.0 nm. The serum samples were diluted 1:4 with zinc-free, triple-distilled water. For a stand ard, pure zinc metal granules (99.9%) were dissolved 1:1 in hydrochloric acid and diluted to 1 liter to give a concentration of 1000/^g/ml (stock). The working stand ards were prepared at concentrations of 0.2, 0.4, and 0.6 Mg/ml of zinc with 10% glycerol solution to match the viscosity of the diluted serum.
Estimation of copper. For estimation, a copper, hollow cathode lamp was used with a lamp current of 3.5 ma. The wavelength was adjusted to 324.7 nm and the spectral band pass to 0.5 nm. The serum samples were diluted 1:1 with triple-distilled water to prevent protein obstruction of the burner head and atomizer. The stock copper stand ard (1000 Mg/ml in 1% HN0 3 ) was procured from Sigma Chemical Company, St. Louis, Missouri, U.S.A. The working stand ards were prepared at concentrations of 1, 2, and 3 ng/m\ of copper using 10% glycerol solution.
The microcomputer facility available in the instrument was used for direct concentration measurement of zinc and copper from the stand ard curves created from the memory.
Statistical analysis. Statistical analysis was carried out by applying Student's t test and Pearson and Lee's correlation coefficient with the help of a computer. The p values below 1% were considered highly significant.
RESULTS
A significant decrease was noticed in the serum zinc levels over the whole spectrum of leprosy, compared to healthy controls, the maximum decrease being seen in LL cases with lepra reaction followed by active LL, BL, and BT cases (The Table). The mean scrum zinc level (126.32 ± 6.98) in cases with ENL reaction receiving oral zinc therapy was significantly higher than the levels of the other patient groups and healthy controls. The differences were highly significant by Student's t test (0.001< p < 0.005).
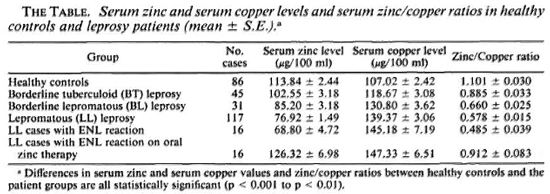
Compared to healthy controls, the mean serum copper levels in all of the groups of leprosy patients were higher and the differences were highly significant (The Table). Maximum increases were found in cases with ENL reaction followed by LL, BL, and BT cases. The mean copper level (147.33 ± 6.51) in cases with ENL reaction on oral zinc therapy was slightly higher than the mean value (145.18 ± 7.19) of active LL cases with ENL reaction, but the difference was not significant.
The zinc/copper ratios (The Table) were greater in LL cases with ENL reaction followed by LL, BL, and BT cases. In all four groups, the differences were highly significant (p < 0.001) when compared to healthy controls. The mean ratio (0.912 ± 0.083) of zinc/copper in LL cases with ENL reaction treated with oral zinc sulfate was close to the mean ratio of the healthy controls (1.101 ± 0.030), which was significantly (p < 0.001) higher than reaction cases not receiving oral zinc therapy. When compared to the LL cases, the zinc/copper ratios of all the other types of leprosy, including ENL reaction cases on oral zinc therapy, were significantly different, with p values between 0.1% and 5%.
The Figure shows a very good negative correlation (r = - 0.998) between mean serum zinc and copper levels from healthy controls to LL cases with ENL reaction.
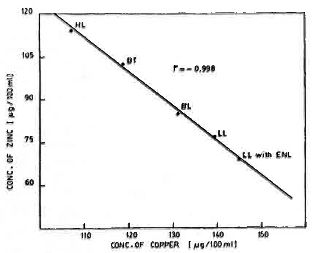
The figure. Scattergram of mean copper and zinc levels in healthy controls (HL), BT, BL, LL cases, and LL cases with ENL reaction.
DISCUSSION
The findings of the present study, significant reduction in the serum levels of zinc and simultaneous increases in the serum levels of copper in leprosy patients across the spectrum of the disease, in general confirm the observations of earlier investigators (8,9,11,30). These differences in the serum levels of the two minerals could reflect the difference between the absorptive processes of the two minerals in the stomach and in the duodenum (29). However, it should be mentioned that the serum copper levels obtained in the present study are slightly lower for both the controls and the patient groups than those reported by earlier workers (8,30). This may be explained by the greater sensitivity of the atomic absorption spectrophotometry used in the present study compared to the colorimetric methods used earlier. It is interesting to note that in the present study a very good negative correlation was obtained between serum zinc and copper levels in the healthy controls and in the LL cases with ENL reaction (The Figure).
Low serum zinc levels have been found in many conditions associated with depressed CMI (6,14). In leprosy, there is a gradual decrease in the serum zinc level (24,30) and depression in CMI from the TT to the LL end of the leprosy spectrum (3,4). It has been suggested that the increasing bacterial load in the macrophages through the leprosy spectrum could produce hypozincemia by increasing the liberation of the leukocyte mediator (LEM)-like substance which stimulates zinc redistribution with hepatic uptake, thus reducing serum zinc concentration (24). Serum zinc deficiency has been reported in alcoholism (26,28) and in cirrhosis of the liver (27). Alteration in liver function in leprosy could be an inducing factor in the very low serum zinc levels observed in those with the disease. Dapsone treatment can also contribute to the reduction of the serum zinc level by competing for protein sites, as suggested by Oon, et al. (13).
As regards the effect of oral zinc therapy in cases with ENL reaction, the serum levels of zinc found in the present study are higher than those reported by Venkatesan, et al. but are comparable to those obtained by Mathur, (10). This could be attributed to a longer oral zinc therapy (6 weeks) in the present study than in the earlier investigation by Venkatesan, et al. (2 weeks). No reduction was noticed in scrum copper levels in cases with lepra reaction receiving oral zinc therapy.
It may be mentioned in passing that the patients included in the present study may have different dietary patterns (regional variations) from those of earlier studies. However, the results indicate that these differences do not affect serum copper and zinc levels in leprosy patients.
Mathur (9,10) have reported beneficial effects, such as faster clinical improvement, rapid fall in the bacterial index (BI), activation of CMI, and low incidence of ENL, when oral zinc was given as an adjunct to conventional leprosy chemotherapy. The optimal duration of zinc therapy, along with careful monitoring of clinical manifestations, CMI-function testing, and serum levels of zinc, may help in understand ing the real significance of oral zinc therapy in leprosy, particularly in ulcerating reactional states.
Acknowledgments. The authors are thankful to Dr. A. V. Paul, CLT&RI, CGL, Chief Médical olficer, and Dr. A. Ramachand ran, Asst. Director (Clinical), for arrangement of patients for the study. The technical assistance of Mr. M. Rajand ran, D. Krishnan, and K. Pand i is gratefully acknowledged. Our thanks arc also due to Mr. S. Scshadri for his secrctarial assistance.
REFERENCES
1. BJORKSTEN, B.,BACK, O.,GUSTAVSON, K. H., HALLMANS, G., HAGGLOF, B. and TARNVIK, A. Zinc and immune function in Down's syndrome. Acta Paediatr. Scand .69(1980)183-197.
2. BRENDSTRUP, P. Serum iron, total iron binding capacity and serum copper in acute and chronic infections. Acta Med. Scand .145(1953)315-325.
3. BULLOCK, W. E. Studies of immune mechanisms in leprosy. I. Depression of delayed allergic response to skin test antigens. N. Engl. J. Med.178(1968)298-304.
4. GODAL, T. Immunological aspects of leprosypresent status. Prog. Allergy 25(1978)211-242.
5. GOLDEN, M.H. N. and GOLDEN, B. E. Trace elements; potential importance in human nutrition with particular reference to zinc and vanadium. Br. Med. Bull. 37(1981)31-36.
6. GOLDEN, M.H. N.,JACKSON, A. A. and GOLDEN, B. E. Effect of zinc on thymus of recently malnourished children. Lancet 2(1977)1057-1059.
7. HUSAIN, S. L. Oral zinc sulphate in ulcers. Lancet 1(1969)1069-1071.
8. KHAIKE, D. S. and MAGAR, N.G. Copper in leprosy-blood plasma concentration and urinary excretion. IndianJ. Med. Res. 60(1972)1697-1701.
9. MATMUR, N.K., BUMB, R. A. and MANGAL, H. N. Oral zinc in recurrent erythema nodosum leprosum reaction. Lepr. India 55(1983)547-552.
10. MATKUR, N.K., BUMB, R. A.,MANGAL, H. N. and SHARMA, M. L. Oral zinc as an adjunct to dapsone in lepromatous leprosy. Int.J. Lepr. 52(1984)331-338.
11.MATHUR, N.K., SHARMA, M.,MANGAL, H. N. and RAI, S. M. L. Serum zinc levels in subtypes of leprosy. Int.J. Lepr. 52(1984)327-330.
12. OLESKE, J. M., WESTPHAL, M. L.,SHORE, S., GORTON, D., BOGDEN, J. D. and NAHMIAS, A. Zinc therapy of depressed cellular immunity in acrodermatitis entcropathica; its correction. Am.J. Dis. Child. 133(1979)915-918.
13. OON, B. B., KHONG, K. Y., GREAVES, M.W. and PLUMMER, V. M. Trophic skin ulceration of leprosy; skin and serum zinc concentrations. Br. Med. J. 2(1974)531-533.
14. PEKAREK, R. S., STANDSTEAD, H. H., JACOB, R. A. and BARCOME, D.F. Abnormal cellular immune responses during acquired zinc deficiency. Am.J. Clin. Nutr. 32(1979)1466-1471.
15. PRASAD, A. S., ed. Trace Elementsand Ironin Human Metabolism. New York: Plenum Press, 1978.
16. PRASAD, A. S. Clinical, biochemical and pharmacological role of zinc. Ann. Rev. Pharmacol. Toxicol.19(1979)393-426.
17. PRASAD, A. S. Trace elements: biochemical and clinical effects of zinc and copper. Am.J. Haematol. 6(1979)77-87.
18. PRASAD, A. S. Role of zinc in humans. Adv. Chem. Ser. 172(1979)197-229.
19. PRASAD, A. S.,MIALE, A.,JR., FARIO, Z., STANDSTEAD, H. H. and SCHULERT, A. R. Zinc metabolism in patients with the syndrome of iron deficiency anaemia, hepatosplenomegaly. dwarfism, and hypogonadism.J. Lab. Clin. Med. 61(1963)537-549.
20. PRASAD, A. S.,MIALE, A.,JR., FARID, Z., STANDSTEAD, H. H.,SCHULERT, A. R. and DARBY, W. J. Biochemical studies on dwarfism, hypogonadism and anemia. Arch. Intern. Med. (Chicago) 111(1963)407-428.
21. RAMU, G. and NAGARAJAN, V. Biochemical investigations in leprosy.J. Indian Med. Assoc. 39(1962)459-464.
22. SAXENA, N.,SHARMA, R. P. and SINGH, V. S. Study of serum zinc levels in leprosy. Indian J. Lepr. 60(1988)556-561.
23.SHANKER, A.,GUPTA, S. B. and SHARMA, J. N. A study of serum and skin zinc in leprosy. IndianJ. Dermatol. Vcnereol. Lepral. 42(1976)258-260.
24. SHER, R.,SHULMAN, G., BAILY, P. and POLITZER, W. M. Serum trace elements and vitamin A in leprosy subtypes. Am.J. Clin. Nutr. 34(1981)1918-1924.
25. SINHA, S. N. and GABRIELI, E. A. Serum copper and zinc levels in various pathologic conditions. Am.J. Pathol. 54(1978)570-577.
26. SULLIVAN, J. F. Effect of alcohol on urinary zinc excretion. Quart.J. Studies Alcohol 23(1962)261-220.
27. SULLIVAN, J. F. and BURCH, A. Potential role of zinc in liver disease. In: Trace Elements in Human Health and Disease. Prasad, A. S. ed. New York: Academic Press, 1976, vol. 1, pp. 67-85.
28. SULLIVAN, J. F. and LANKFORD, H.G. Zinc metabolism and chronic alcoholism. Am.J. Clin. Nutr. 17(1965)57-63.
29. VAN CAMPEN, D. R. Effects of zinc, cadmium, silver and mercury on the absorption and distribution of copper-64 in rats.J. Nutr. 88(1966)125-130.
30. VENKATESAN, K., KANNAN, K. B.,BHARADWAJ, V. P.,SRITHARAN, V., KATOCH, K., USHA, R. and RAMU, G. Serum copper and zinc in leprosy and effect of oral zinc therapy. Indian J. Med. Res. 78(1983)37-41.
1. M.Sc, Research Officer, Department of Biochemistry; Central Leprosy Teaching and Research Institute, Chengalpattu, Tamil Nadu 603 001, India.
2. M.D., Director (Microbiology), Central Leprosy Teaching and Research Institute, Chengalpattu, Tamil Nadu 603 001, India.
3. M. Sc., Ph.D., Head, Department of Biochemistry; Sacred Heart Leprosy Centre, Kumbakonam, Tamil Nadu 612 401, India.
4. M.D., Senior Physician, Sacred Heart Leprosy Centre, Kumbakonam, Tamil Nadu 612 401, India.
Reprint request to Dr. Ramu.
Present address for Joseph George, M. Sc.: Department of Biochemistry, Central Leather Research Institute, Adyar, Madras 600 020, India.
Received for publication on 22 February 1990.
Accepted for publication in revised form on 23 August 1990.