- Volume 59 , Number 1
- Page: 116–9
Intralesional variations f rom lepromatous to tuberculoid histology - a case report*
Editor's Note: In an effort to increase the utility of the JOURNAL in continuing medical education, it has been suggested that a new feature of the JOURNAL be added on a trial basis to the Editorial Section-Clinical Notes. In this section, we welcome contributions dealing with practical problems in leprosy work. Submissions to this section will undergo minimal editorial changes and may well contain controversial points. Letters to the Editor pointing out other viewpoints are welcome. - RCH
Leprosy, classified according to Ridley and Jopling,1 forms a spectrum ranging from the localized tuberculoid to the generalized lepromatous disease with an array of borderline manifestations between the two polar types, depending on the immunological state of the patient. Instances of histopathological changes of borderline tuberculoid leprosy existing in one lesion and changes of lepromatous leprosy in another lesion in the same patient have been observed. 2 We report a patient having histopathological appearances of both borderline lepromatous and tuberculoid histology in the same lesion.
Case report. The patient was a 10-year-old male from the South Pacific island of Pohnpei, who presented with a hypopigmented skin lesion on the back. On examination, a nodule was also seen on the upper part of the right leg. A punch biopsy, including the subcutaneous tissue, was obtained from the nodule, was fixed in 10% buffered Formalin, and was sent to us for histopathological study. No other details were available to us from the clinical record.
The biopsy was processed for paraffin sections, 5 μ-thick sections were made and stained with hematoxylin and eosin and a modified Fitc stain. 3 The sections showed skin and subcutaneous tissue (Fig. 1). There was granulomatous inflammation occupying nearly 80% of the tissue. The epithelium showed minimal acanthosis and parakeratosis. A thin clear zone separated the granuloma from the epidermis in most areas, but in some spots the granuloma reached up to and infiltrated the epidermis. The upper one third of the dermis was replaced by a granuloma composed of a sheet of macrophages (Fig. 2), some of which were spindle shaped. A few had a foamy cytoplasm. An occasional, poorly formed, foreign body giant cell and very few lymphocytes were also present among them. The middle one third of the granuloma on careful examination showed some increase in lymphocytes and epithelioid cells. The arrectorcs pilorum muscle cells and other skin adnexa were infiltrated by the granuloma. A remnant of a nerve bundle was present in the midst of a granuloma (Fig. 3). The deeper one third of the granuloma, involving the deep dermis and the subcutaneous tissue, showed well-formed tubercles with central areas of epithelioid cells surrounded by numerous lymphocytes (Fig. 4). No nerve tissue was identified in this area.

Fig. 1. Photomicrograph of entire histopathological section of the biopsy showing borderline lepromatous granuloma at upper dermis and tuberculoid granuloma at deep dermis and subcutaneous tissue (H&E x 20).
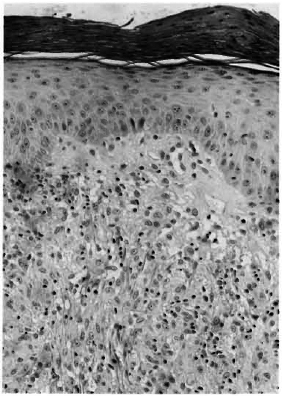
Fig. 2. Photomicrograph showing clear zone separating epidermis from the macrophage granuloma (H&E x 120).

Fig. 3. Photomicrograph showing remnant of a partly destroyed nerve inside a tuberculoid granuloma (H&E x 120).
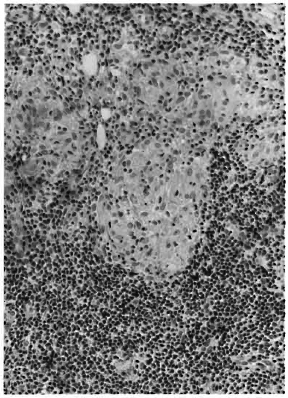
Fig. 4. Photomicrograph showing a focus of epithelioid cells surrounded by dense collections of lymphocytes characteristic of a tuberculoid granuloma (H&E x 120).
Acid-fast staining showed bacilli to a load of 3+ to 5+ (Fig. 5) in the upper one third of the granuloma. They were seen in clumps inside macrophages and the arrectorcs pilorum muscle cells. The nerve tissue partly destroyed by the granuloma did not show any organisms. An occasional bacillus was present inside cells in the middle one third of the granuloma to a load of 1+. In the deeper parts of the granuloma there were no organisms.
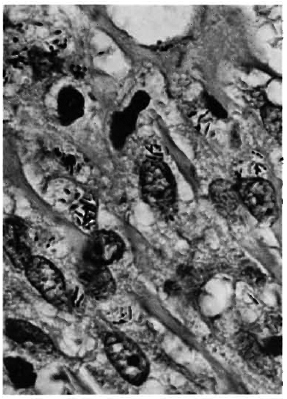
Fig. 5. Photomicrograph showing clumps of acid fast organisms inside macrophages (acid-fast stain x800).
Comment. Small foci of epithelioid cells in the midst of a lepromatous granuloma have been shown in lepromatous patients undergoing immunotherapy4 and in the subcutaneous nodules of some histoid leprosy patients. 5 In this biopsy, histopathological changes consistent with borderline lepromatous leprosy were seen in the upper one third of the dermis and tuberculoid disease was seen in the deeper portion of the dermis and subcutaneous tissue. To our knowledge, this phenomenon of finding divergent histopathological changes in the same lesion with such clear demarcation has not been documented. It is difficult to explain such an occurrence according to the spectral concept of the disease. Meager clinical information and the lack of laboratory data in this case make it more difficult. Is it possible that this presentation could be either an upgrading or a downgrading reaction in borderline leprosy?6 Ordinarily the histopathological changes signifying an upgrading or a downgrading reaction will be present diffusely throughout the granuloma, unlike what was seen in this lesion where the tuberculoid transformation was mostly confined to deeper portions of the lesion and the borderline lepromatous granuloma was present only in the superficial dermis.
Srinivasan, et al. 7 have examined simultaneous biopsies from the skin and cutaneous nerves from 36 patients and 21 of them showed dissimilarities in the histopathological appearances between the two sites. In one patient this was even to the extent of manifesting a BT/TT response in the skin with no bacilli and BL in the nerves with numerous bacilli. 7 Similar variations in the histopathological responses involving nasal mucosa, nerve, and skin have also been reported by Chacko. 8 Srinivasan, in an interesting exposition, attempts to explain the simultaneous occurrence of different types of leprosy in different lesions in the same patient by the "cusp catastrophic model for leprosy. " According to this theory, the variation in manifestation in the same patient is an instance of "divergence" where the lesions are similar to begin with but, as they progress, they show different forms under similar conditions of change. 9
Finally, the importance of performing a biopsy deep enough to include the subcutaneous tissue cannot be overemphasized. In this patient, if a superficial biopsy had been obtained a diagnosis of borderline lepromatous leprosy would have been offered, and the tuberculoid response in the deeper tissue would have been completely missed.
Summary. A patient showing simultaneously in one lesion clearly demarcated histopathological changes consistent with borderline lepromatous and tuberculoid leprosy is described. To our knowledge, this is the first recorded case of such an unusual histopathological appearance.
- Charles K. Job, M. D., F. R. C. Path,
Vernia Drain, M. D.
Pathology Research Department
- Robert R. Jacobson, M. D., Ph. D.
Chief, Clinical Branch
- Robert C. Hastings, M. D., Ph. D.
Chief, Laboratory Research Branch
GWL Hansen's Disease Center
Carville, Louisiana 70721, U. S. A.
Ackowledgment. We are grateful to Mr. John Marcell for the technical work, Mr. Gregory T. McCormick for assistance in photomicrography, and Ms Mary Lee M. Jackson for typing the manuscript.
1. Ridley, D. S. and Jopling, W. H. Classification of leprosy according to immunity; a five-group system. Int. J. Lepr. 34(1966)255-273.
2. Ganapati, R. and Dcsikan, K. V. Simultaneous occurrence of lesions of different types of leprosy in a patient-a case report. Lepr. India 46(1974)148-151.
3. Job, C. K. and Chacko, C. J. G. A modification of Fite's stain for demonstration of M. leprae in tissue sections. Indian J. Lepr. 58(1986)17-18.
4. Hastings, R. C. and Job, C. K. Reversal reactions in lepromatous leprosy following transfer factor therapy. Am. J. Trop. Med. Hyg. 27(1978)995-1004.
5. Wade, H. W. and Tolentino, J. G. The histoid variety of lepromatous leprosy. Int. J. Lepr. 31(1963)608-609.
6. Ridley, D. S. and Job, C. K. The pathology of leprosy. In: Leprosy, Hastings, R. C, ed. New York: Churchill Livingstone, 1985, pp. 111-133.
7. Srinivasan, H., Rao, K. S. and Iyer, C. G. S. Discrepancy in the histopathological features of leprosy lesions in the skin and peripheral nerve; report of a preliminary study. Lepr. India 54(1982)275-282.
8. Chacko, C. J. G. Evolution of pathological lesions in leprosy patients. (Abstract 0-24) In: Abstracts of Scientific Papers of the XVI Biennial Conference of the Indian Association of Leprologists, Trichur, India, 1989.
9. Srinivasan, H. Models for leprosy. An appraisal of graphic representations of the "spectrum" concept as models and a suggestion for a catastrophic theory model for leprosy. (Editorial) Int. J. Lepr. 52(1984)402-413.
*Wayne M. Meyers, M. D., Ph. D., kindly served as Editor in regard to the submission, review, revision, and acceptance of this manuscript.