- Volume 59 , Number 1
- Page: 122–4
Therapeutic implications of morphological study of nerves f rom treated or untreated tuberculoid or lepromatous leprosy*
To the Editor:
In view of the overoptimism prevailing in several parts of the world, especially in India, and to dispel misleading notions of eradicating or curing leprosy by the year 2000, it is considered essential to publish, even as Correspondence, our light- and electron-microscopic findings on 27 nerve biopsy specimens referred to us by a variety of clinical specialists, notably neurologists, dermatologists, internists, and plastic surgeons. These were totally unsolicited rand om cases sent to us for nerve biopsy examination in view of nearly 40 years of interest in and work on leprous neuritis by one of us (DKD).
A third of the biopsies (9) were from patients who had leprosy already diagnosed, several months to years earlier, by clinical and /or skin biopsy examination (see table below). Approximately another third of the biopsies were from patients with leprosy suspected for the first time from clinical signs or sensory-motor neuropathy, generally with some thickening and tenderness of the large nerve trunks, and with or without EMG examination showing the same. The remaining third of the biopsies were referred to us from cases with vague sensory signs and symptoms of totally unclear etiology. The latter two groups did not have any skin patches.
The biopsy was invariably taken from one sural nerve at and just above the ankle. The specimen was collected in the operating room, and divided for different morphological studies by a member of our laboratory. This included Formalin fixation for variably stained paraffin sections and, in a few cases, for immunohistology for S-100 protein; in a chilled dry vial for histochemistry (lysosomal enzymes) on frozen sections; and in glutaraldehyde for semithin and ultrathin sections for light- and electron-microscopy, respectively.
We have earlier reported clinical and pathological changes with the persistence of Mycobacterium leprae on light- and electron-microscopy in nerves from lepromatous patients long treated with dapsone, now seen occasionally even after multidrug therapy (MDT). We have further been impressed by the development, or clinical recurrence after initial improvement, of peripheral nerve changes including active inflammatory reaction, in MDT-administered patients even of the paucibacillary or tuberculoid type. In a period under 2 years, the eight treated tuberculoid cases have shown nerve-damaging changes, with no detectable acid-fast bacilli (AFB) by routine methods but occasional bacilli on electronmicroscopy. There was moderate loss of myelin and axons, good expression of S-100 protein in the remaining Schwann cells, and replacement fibrosis in nerves from both the treated tuberculoid and treated lepromatous cases. In lepromatous patients with their inherent lepromin negativity, i. e., severe deficiency of cell-mediated immunity (CMI), and the excessive bacillation in the pretreatment state, multiplication of the remaining bacilli in Schwann cells and continued damage to nerves is almost expected. More surprising and dangerous for society is the persistence or recurrence of inflammatory reaction and nerve damage, with very few or no AFB, in treated tuberculoid patients with good inherent CMI where delayed-type hypersensitivity to minimal M. leprae antigen or a nonbacillary antigen, such as myelin basic protein from damaged nerves, must be considered.
This whole set of observations, important for the patients and for the general population, would have been impossible without adequate nerve biopsies. We have considered skin biopsies not only inadequate but misleading when negative for bacilli and not showing intradermal nerve changes. Particularly in oncc-proven lepromatous leprosy, one of us (DKD) has considered the withdrawal of treatment, even a few years later and after repeated negative skin biopsies, to be a potentially dangerous practice since the disease may be remaining clinically dormant with the infection persisting in the nerves (1). Hence, we strongly endorse Jacob and Mathai's plea (4) for a nerve biopsy. Having now observed the more subtle danger of paucibacillary tuberculoid leprosy showing very severe nerve-damaging changes (Fig. 1) after many years of apparently successful chemotherapy (cither dapsone or MDT), the report of Grugni, et al. (2) and others showing relapses in paucibacillary patients after MDT is not at all surprising.
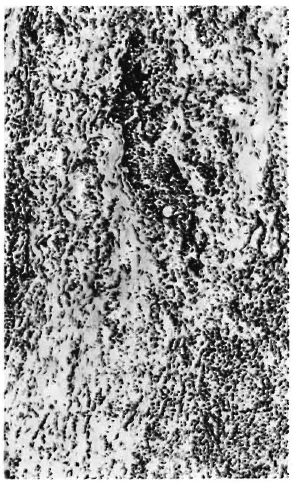
Fig. 1. (NP/201/90): M/41 years; neuritic leprosy diagnosed December 1985; treated with dapsone, clofazimine, deltacortil for 2 years; 1987 = skin biopsy elsewhere, reported as regressing tuberculoid leprosy; April 1990 = nerve trunks of all four limbs thickened and hard to feel, total analgesia feet R > L, and pain in both legs. Sural nerve biopsy.
Longitudinal section of entire nerve bundle from this treated tuberculoid patient, showing destruction by active inflammatory and fibrotic reaction. Inflammatory cells are mainly lymphocytes with some large mononuclear cells in foci and scattered. Small fusiform nuclei belong to remaining Schwann cells and proliferated fibroblasts (H&E on frozen section, x 75).
Finally, we would urge the use of S-100 antibody, in the usual peroxidase-antiperoxidase procedure on paraffin sections, on nerve biopsies and skin biopsies for all types of leprosy-in nerve biopsies to detect the remaining intact Schwann cells in otherwise destroyed nerve bundles, as we have done (Fig. 2); in skin biopsies to detect the remnants of nerve fibers in granulomas, as elegantly demonstrated by Job, et al. (3).
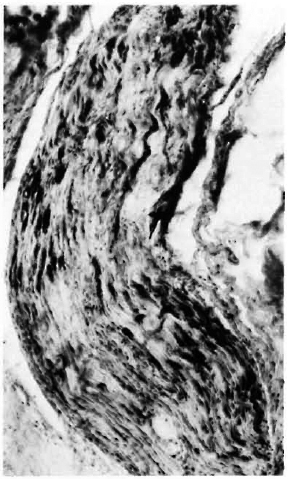
Fig. 2. (NP/551/89): M/50 years; diagnosed leprosy from hypopigmented anesthetic patches on all fourlimbs 15 years ago (1974). Treated for 10 years (1979-1989) with dapsone, rifampin and edinol; while stillon this MDT, hypalgesia developed in both lateral pop-liteal nerve territories, very thickened ulnar, lateralpopliteal and radial cutaneous nerves detected withmild hand muscle weakness. Sural nerve biopsied Sep-tember 1989.
Longitudinal section of a nerve bundle from this treated tuberculoid case showing short, dark, parallelrunning band s of remaining Schwann cells reacting to S-100 protein. Inflammatory reaction was lesser and endoneurial fibrosis greater in this case than in Fig. 1 case (PAP reaction using S-100 antibody on paraffin section, x75).
- Dara b K. Dastur, M. D., D. Sc. (Bom. ),
F. R. C. Path. (Lond. ), F. A. M. S., F. N. A.
Daya K. Manghani, Ph. D. (Bom. ),
Ph. D. (Lond. )
Jeroze F. Elavia, B. Sc.
Department of Neuropathology and Applied Biology
MRC-15th Floor
Bombay Hospital
Bombay 400020, India
REFERENCES
1. DASTUR, D. K. Pathology and pathogenesis of predilective sites of nerve damage in leprous neuritisnerves in the arm and the face. Neurosurg. Rev. 6(1983)139-152.
2. GRUGNI, A., NADKARNI, N. J., KINI, M. S. and MEHTA. V. R. Relapses in paucibacillary leprosy after MDT-a clinical study. Int. J. Lepr. 58(1990)19-24.
3. JACOB, M. and MATHAI, R. Diagnostic efficacy of cutaneous nerve biopsies in primary neuritic leprosy. Int. J. Lepr. 56(1988)56-60.
4. JOB, C. K., DRAIN, V., DEMING, A. T., HASTINGS, R. C. and GERBER, M. A. Role of S-100 protein as a marker for Schwann cells in the diagnosis of tuberculoid leprosy. (Letter) Int. J. Lepr. 58(1990)392-393.
*Abstract of talks given at: a) Workshop W. S. 1 on Tropical Neurological Diseases, XI International Congress of Neuropathology, Kyoto, Japan, September 1990 (Chairmen: Prof. D. K. Dastur and Prof. Itakura), and b) Workshop W. S. 2. 9 on Infectious Neuropathies, VII International Congress on Neuromuscular Diseases, Munich, Germany, September 1990 (Chairmen: Prof. D. K. Dastur and Prof. G. Said).