- Volume 58 , Number 4
- Page: 717–9
Cervical perineurial cyst, a red herring (Case Report)
ABSTRACT
Leprous mononeuropathy may present without demonstrable maculoanesthetical patches. A case is described in whom wasting of the right hand was initially attributed to C8 Tl entrapment radiculopathy caused by cervical perineurial cysts. On the basis of the benign nature of the perineurial cysts and questionable right ulnar nerve thickening, the patient was given a trial of antileprosy drugs. A follow-up clinico-electrophysiological evaluation favored the diagnosis of leprotic ulnar mononeuropathyEditor's Note: In an effort to increase the utility of the JOURNAL in continuing medical education, it has been suggested that a new feature of the JOURNAL be added on a trial basis to the Editorial Section-;Clinical Notes. In this section, we welcome contributions dealing with practical problems in leprosy work. Submissions to this section will undergo minimal editorial changes and may well contain controversial points. Letters to the Editor pointing out other viewpoints are welcome.-RCH
Intraspinal cysts may be located outside or inside the dura mater. They are detected incidentally during myélographie or spinal CT studies and are usually benign. Intradural perineurial cysts are seen in the sacral area and, rarely, in the cervical or thoracic regions.1-3 Perineurial cysts mostly arise at the site of the posterior root ganglion, and their wall is composed of neural tissue. These cysts are differentiated from meningeal cysts/ diverticula by their location along the nerve root, delayed filling with the contrast medium, and microscopic features.2 Occasionally, these cysts may become symptomatic and cause compressive myeloradiculopathy. We present a young man who had progressive wasting of the right hand caused by neuritic leprosy which, in the absence of any hypoesthetic skin lesion, was attributed to compression of the cervical roots by the perineurial cysts in their early course. Prolonged F-wave latency attributable to motor radicle involvement and nerve conduction studies correlated well with the clinico-radiological diagnosis of entrapment radiculopathy by the perineurial cysts. However, antileprosy drugs were started on the basis of mild ulnar nerve thickening across the medial epicondyle, and surgery was postponed. The clinical course and nerve conduction studies 6 months later confirmed neuritic leprosy as the underlying disease.
CASE REPORT
A 29-year-old, nondiabetic male (a tailor by profession) presented with a history of progressive wasting of the right hand for 1 year. He denied fasciculations, sensory loss, any febrile episodes, and any history of trauma. General and systemic examination was normal. There was a partial clawing deformity of the right hand. Hypothenar and the interossei muscles were more wasted compared to the thenar group of muscles. The power in the right dorsal and palmar interossei, lumbricals, abductor digiti minimi, and adductor pollicis brevis muscles was reduced by 30% to 50%. A subjective sensory impairment of pain and temperature was observed over the dorsal and palmar surfaces of the medial two fingers and the right forearm. However, there was no objective sensory loss or hypoesthetic hypopigmented skin patch. All deep and superficial reflexes were normal. The right ulnar nerve across the medial epicondyle was minimally thickened compared to the left side. Hemogram, blood biochemistry, plain x-ray of the cervical spine, and cerebrospinal fluid were normal. In view of progressive asymmetric wasting of the right hand, an iohexol lumbar myelogram was done which showed free flow of dye across the cervical region. There was filling of multiple bilateral cysts placed across the 5th, 6th, 7th, and 8th cervical roots (The Figure). The contrast medium could be dislodged partially by positioning the patient. The largest cyst (about 15 mm in diameter) was seen in relation to the right 7th cervical foramen transversarium. Its placement outside the intervertebral foramen was confirmed in an iohcxol spinal CT x-ray (The Figure).
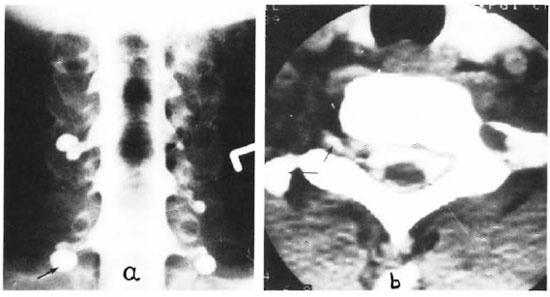
The Figure. Multiple cervical perineurial cysts seen on a) iohexol myelogram and b) iohexol spinal CT scan with largest cyst over C8 radicle (large arrow).
Right ulnar motor nerve conduction studies revealed a mild increase in distal latency of 5 milliseconds (ms), normal nerve conduction velocity of 50 m/sec, and prolonged F-wave latency of 44.4 ms, suggesting a proximal lesion in the nerve trunk or radicle. Ulnar sensory nerve conduction showed a mild abnormality in the form of reduced amplitude of the sensory action potential (14 nv) as compared to 21 nv in the opposite ulnar nerve. Skin biopsies from the forehead, right ear lobule, and medial dorsum of the right hand did not reveal bacteriological or morphological evidence of leprosy. He was started on a daily dose of 100 mg of dapsone and 600 mg of rifampin. Six months later he was observed to have a well-defined, 10-cm diameter anesthetic patch over the dorsum of the right hand. However, the wasting was static although subjectively he felt improvement in hand grip. A follow-up right ulnar motor conduction revealed a distal latency of 4.8 ms; nerve conduction velocities (NCV) of 38 m/sec in the forearm, 35 m/sec in the arm, and 28.5 m/sec across the elbow. Results of a right ulnar F-wave wrist latency and an EMG study of the right abductor digiti minimi were the same as before.
DISCUSSION
This patient presented with a wasted hand. A myelogram and a spinal CT revealed multiple intraspinal cystic swellings in the cervical region. Their communication with the spinal subarachnoid space and extradural location was confirmed. The wasting of the intrinsic muscles of the right hand could have been attributed to compression of a mixed trunk of C8 motosensory radicles by the largest cyst placed near the 7th right foramen transversarium. This was substantiated by ulnar motor nerve conduction studies which showed gross asymmetry of F-wave latency and a marginal increase of distal latency suggestive of motor radicle involvement.4 Since perineurial cysts are rarely symptomatic and the ulnar nerve was slightly thickened, the patient was given the benefit of the doubt of leprous mononeuropathy. Follow-up observations of the anesthetic patch over the right dorsum of the hand, the fall of motor nerve conduction velocities, and the minimal improvement in the motor deficit leaves little doubt regarding the diagnosis of leprosy. Repeat skin biopsies from the forehead, ear lobule, and right hand anesthetic patch were negative for leprosy bacilli. Our patient probably had paucibacillary (tuberculoid) leprosy, a form of leprosy in which skin biopsies are usually negative for leprosy bacilli. Retrospectively, the increase in the F-wave latency during the first examination can be explained on the basis of ulnar nerve involvement in the right arm above the medial epicondyle where it lies superficially and is prone to leprosy affection.
- S. K. Bansal, M.D., D.M.
U. K. Dhand, M.D., D.M.
Department of Neurology
- N. Khandelwal, M.D.
Department of Radiodiagnosis
- J . S. Chopra, D.Ch., F.R.C.P., Ph.D., F.A.M.S.
Department of Neurology
Postgraduate Institute of Medical Education and Research
Chandigarh 160012, India
1. Holt, S. and Yates, P. O. Cervical nerve root "cysts." Brain 87(1964)481-490.
2. Tarlov, I. M. Spinal perineurial and meningeal cysts. J. Neurol. Neurosurg. Psychiat. 33(1970)833-843.
3. Wilkins, R. H. Intraspinal cysts. In: Text Book of Neurosurgery. Wilkins, R. H. and Rengachary, S. S., eds. New York: McGraw-Hill Book Company, 1985, pp. 2061-2063.
4. Brown, W. F., Ferguson, G. G., Jones, M. W. and Yates, S. K. The location of conduction abnormalities in human entrapment neuropathies. Can. J. Neurol. Sci. 3(1976)111-122.