- Volume 58 , Number 2
- Page: 381–2
Lepromatous leprosy and dementia
To the Editor:
I would like to report a patient who was believed to suffer from a depressive reaction following the onset of cutaneous lesions of leprosy but whose cognitive impairment was found to be associated with the systemic diseases, diabetes mellitus and cerebral atrophy.
A 57-year-old Chinese male was brought to the skin clinic in March 1989 with a history of skin nodules and reactive depression of 2 years' duration. He was uncooperative but not abusive or aggressive. His appetite was good but he suffered from insomnia. There was no history of head injury, diabetes mellitus, or mental illness in the family. He was not an alcoholic but smoked about 10 cigarettes a day for 30 years. He had isolated himself and had wandered aimlessly clad in his underpants. The skin lesions were that of leprosy. He appeared in good health but was withdrawn, dull, fearful, depressed, showed a lack of emotional response, and was dressed carelessly. His speech was slow and sometimes incoherent, suggestive of impairment of intellectual functions. He had a memory defect for recent events so much so that he ate several times a day forgetting that he had taken food a few hours ago. There were no florid symptoms such as hallucinations or delusions.
His blood pressure was 110/80 mm Hg, and he had 2+ glycosuria. A slit-skin smear for acid-fast bacilli showed a bacterial index (BI) of 5.8+ and a morphological index (MI) of 4.5%. A skin biopsy confirmed the diagnosis of lepromatous leprosy. The results of a modified glucose tolerance test were: Fasting 17.4 mmol/L (normal 3.6-6); 1 hr 26.6 mmol/L (normal 10); 2 hr 23.6 mmol/L (normal 6.7). A venereal disease research laboratory (VDRL) test was non-reactive. A radiograph of the chest and other relevant investigations were normal or within normal limits. A computerized tomography (CT) scan of the brain showed features of bifrontal atrophy (The Figure). He was treated with chlorpromazine, gliben-clamide and multidrug therapy (MDT) for multibacillary leprosy. The hyperglycemia was fairly well brought under control, and he was able to sleep well. He did not talk with other patients in the ward, was difficult with medication, and did not follow instructions in his diabetic diet. There was an improvement in mood, in that he was quite cheerful and was able to smile during follow up. His disorientation in space and time was less evident than before.
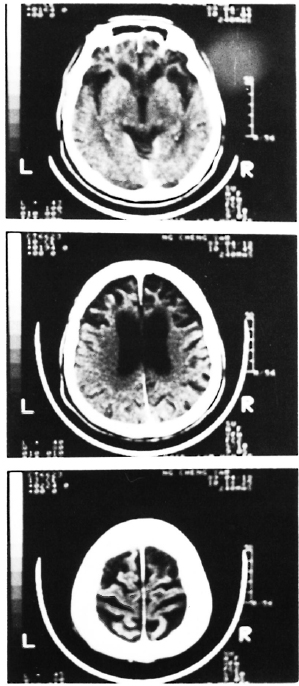
The Figure. Contrast-enhanced computerized tomography (CT) scan of the brain showing dilatation of the lateral ventricles and prominent sulci predominantly in both the frontal and parietal lobes.
Dementia is a chronic organic brain syndrome which involves the intellect, memory, emotions, and behavior whose decline exceeds that expected of normal aging. The degree of deterioration depends upon the various causes (3), such as cerebral arteriosclerosis, trauma, tumors, endocrine disturbances, intoxication and deficiency disorders, and a group of degenerative diseases which include Alzheimer's disease. Pick's disease, Huntington's chorea, and senile dementia. The classification of dementia is disputed and takes into account different variables (2) such as the etiology, age at onset, pathology, etc., but the subcortical-cortical dichotomy seems to supersede that of the previously held senile and presenile dementia. Fluctuations in mood -euphoria and depression -are common in this disease. However, depression in dementia should be differentiated, which is not easy, from depressive illness and depressive reaction (4). Presumably, diabetes mellitus might have contributed indirectly to the dementia in our patient through an arteriosclerotic mechanism. Although suicides have been recorded in leprosy patients (5), psychosocial disorders in them are similar to that encountered in patients with other illnesses (1). Nevertheless, overt psychiatric symptoms in these patients should be studied in depth and, if necessary, further investigated so that treatable causes of dementia are not overlooked.
" Dementia and other organic syndromes... provide the clearest example of a relationship between disorders of the mind on one hand and physical or cerebral diseases on the other; a relationship seen in some measure throughout the medical practice" (3).
- Kader N. Mohamed, M.B.B.S., Dip.Derm., Dip.Ven.
Department of Dermatology
General Hospital 10990
Penang, Malaysia
Acknowledgment. My thanks go to the Director-General of Health, Malaysia; Dr. V. Thomas, Consultant Psychiatrist; Dr. Samuel Easaw, Consultant Neurologist; and Mrs. Yahaya Mahmud.
REFERENCES
1. Bahlinger, V. M., Brantley. P. J., Madrigal, D. R., Heroman. M.W. and Veitia. M.C. Psychological stress in Hansen's disease: a comparison with other chronic illness patients. Int. J. Lepr. 53(1985)251-254.
2. Chui. H. C. Dementia; a review emphasizing clin-icopathologic correlations and brain-behaviour relationships. Arch. Neurol. 46(1989)806-814.
3. Roth. M. and Myers. D. H. The diagnosis of dementia. In: Contemporary Psychiatry. Silver-stone, T.. Barraclough, B., eds. Ashford, Kent: Headley Brothers Ltd.. 1975. pp. 87-99.
4. Slater. E. and Roth. M. Clinical Psychiatry. London: Bailliere Tindall, 1977. pp. 188-222.
5. Zhou, D.. et al. [On suicide among leprosy patients.] China Lepr. J. 3 (1987) 240-243. English abstract in Int. J. Lepr. 56(1988)489.