- Volume 58 , Number 3
- Page: 579–88
News and notes
This department furnishes information concerning institutions, organizations, and individuals engaged in work on leprosy and other mycobacterial diseases, and makes note of scientific meetings and other matters of interest.
1989 DAMIEN-DUTTON AWARD
Father Joseph J. Walter, S.J., Executive Director of CMMB (left), accepts the 1989 Damien-Dutton Award from Fr. John V. Tunny, Pastor of St. Joseph's Church, Hewlett, New York, U.S.A. Fr. Walter has around his neck a ribbon with a smaller version of the medallion.
The Damien-Dutton Award for 1989 was presented on 10 November to the Catholic Medical Mission Board (CMMB) in recognition of more than 60 years of providing medical aid and support to the missions of the world, including the poorest of the poor, the victims of leprosy. Father Joseph J. Walter, S.J., CMMB's Executive Director, accepted the honor on behalf of the staff and the many benefactors. In his remarks, Father Walter said that CMMB was especially honored to be designated in 1989, the year of the 25th anniversary of the foundation of the Damien-Dutton Award and the 100th anniversary of the death of Father Damien de Veuster, who died of leprosy at the age of 49 (15 April 1889).
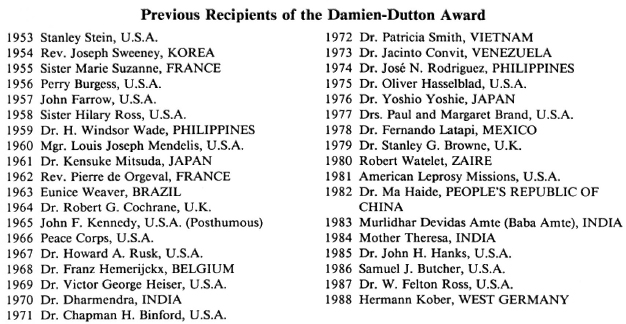
The Award was established in 1953 by the Damien-Dutton Society (founded in 1944 by Mr. Howard E. Crouch) to honor those who have rendered outstanding service to the cause of leprosy.
Belgium. FOPERDA's 50th anniversary. The Father Damien Foundation for the Campaign Against Leprosy (FOPERDA) in Belgium celebrated its 50th anniversary at the end of last year, and to mark the .occasion has published a pamphlet on the formation of the organization and its link to Father Damien.
In 1936 his remains were returned to Belgium. Shortly after, under pressure from admirers of the work of Father Damien, including apparently an active group in Britain headed by the Prince of Wales, it was decided to form an international institution against leprosy. FOPERDA was established as an "établissement d'utilité publique" by Royal Decree on 23 November 1939. Since then it has been active especially in Africa. In the Haut-Uele area of Zaire, FOPERDA has developed over the past 50 years one of the classic models of leprosy control, since copied in many other places.
The booklet can be obtained from: FOPERDA, 16 rue Stevin, 1040 Brussels, Belgium.-ilep FLASH 2 (1990) 3.
Ethiopia. Physician needed at ALERT. The All Africa Leprosy and Rehabilitation Training Centre (ALERT) has need of a medically qualified hospital physician with three years' acceptable experience in general practice, experience in leprosy work preferable. The successful candidate is expected to take part in clinical research activities and training for a contract period of two years. Salary negotiable. Deadline for submitting application is one month after the first publication of this vacancy. Address application with copies of testimonials and job certificate in English to: Executive Director, ALERT, P.O. Box 151, Addis Ababa, Ethiopia.
Guinea-Bissau. Pope celebrates World Leprosy Day. On Sunday, 28 January, Pope John Paul II was present at Cumura, Guinea-Bissau, a project supported by ILEP's Italian member, AIFO, for the celebration of World Leprosy Day. The Pope used the occasion to make a strong appeal on behalf of people with leprosy. Also present was Guido Barbera, Vice-President of AIFO.
The Pope also recently gave a private audience to AIFO personalities together with Dr. Maria Leide, Director of the division in the Brazilian Ministry of Health responsible for the national leprosy program, on the occasion of the presentation to the Mor-hans Project in Brazil of the 1990 Follereau Prize, which is worth approximately $8,000.-ilep FLASH 2 (1990) 2.
India. Bombay Leprosy Project Report of Activities: 1976-1989. To combat the increasing public health problems caused by leprosy in Bombay, the German Leprosy Relief Association (GLRA), West Germany, started financing a field project, namely, the "Bombay Leprosy Project," in 1976. Gradually, the field operation area has been extended to cover a total population of 1.8 million (estimated in 1988). The project is operating 23 clinics, including clinics situated in general hospitals outside the project area. The project is also running a 20-bed hospital. The current objectives of the project are: a) Case detection work through intensive surveys of schools and slums and examination of contacts within the project area by trained medical and paramedical teams; b) starting several treatment centers, especially in slum areas; c) initiating mass health education campaigns to educate the public and also to remove popular misconceptions about leprosy; d) promoting and encouraging study and research work in leprosy and allied sciences; c) imparting field teaching in leprosy to undergraduate and postgraduate medical students; and f) to propagate and practice integration of leprosy patients with society and to run an integrated training and employment program for cured leprosy patients and other handicapped persons with a view to make them self reliant and easily assimilable in society. - From the report.
LEPRA launches sister organization in India. The launch of Lepra-India, an Indian society dedicated to the eradication of leprosy, makes a return to its original focus for Lepra-the British Leprosy Relief Association. Founded in 1924 as the British Empire Leprosy Relief Association, much of the early work supported by Lepra was carried out in India, following an appeal to Indians by the then Viceroy, Lord Reading. This brought in about Rs. 40 lakhs; a sum not matched by an appeal in Britain until some 40 years later.
The inaugural meeting of Lepra-India was held in Hyderabad on 3 August 1989. In a new agreement with the Indian government, Lepra will channel more than Rs. one crore through Lepra-India for leprosy prevention, detection and cure this year. The managing committee of the new society consists of seven eminent Indian trustees and three representatives of Lepra from Britain. Lepra-India is chaired by Dr. K. V. Desikan, a former director of the Japan Asia Leprosy Mission Association (JALMA). Mr. Tilak S. Chauhan is the Chief Executive and cx-officio Secretary of the Society.
India, with an estimated four million leprosy sufferers, has one of the highest incidence rates in the world. Lepra-India's own programs will concentrate on providing multidrug therapy -the most effective treatment, as recommended by the World Health Organization (WHO)-in five of the country's worst affected districts, in partnership with government health services. These are two districts of Andhra Pradesh, two in Orissa, and one in Karnataka.
Inaugurating the Lepra Society-Hyderabad Project, Prof. J. L. Turk, Chairman, Medical Advisory Board LEPRA-U.K., congratulated for launching the project in a record time of 2 weeks. This was possible because of the cooperation of the government of India, state government and various voluntary organizations who engaged in the Leprosy Eradication Programme.
Prof. Turk said that the multidrug therapy is a sure treatment with very negligible lapse and reoccurrence, and the project is first of its kind in an urban area in a period of 5-8 years with an annual expenditure of over 15 lakhs of rupees for detecting the leprosy patients, treatment and rehabilitation. The professor further said that anti-leprosy vaccine can play a vital role in arresting the spread of leprosy and said that we should visualize the conditions beyond 2000 A.D.: disability control program, nerve repair, muscle craft techniques, etc.
Dr. G. V. Nagabhushana Rao, Director, Medical Health Service, A.P., who was the chief guest underlined the importance of multidrug therapy and health education, besides being cautious of reappearence of the disease by continuous evaluation. He said that in A.P. over 50 voluntary organizations are working for the eradication program.
Dr. Desikan, Chairman, Lepra Society, who presided, said that the project is the first of its kind in an urban area like Hyderabad, and thanked the state authorities for cooperating in launching the program. He said that research should continue to avoid self resistance to MDT. He gave a brief report about the leprosy eradication program in Srikakulam and Vizag where the prevalence rate was reduced from 15 to 2 per 1000, which was a spectacular achievement.
Earlier Mr. Tilak Chauhan, Chief Executive of Lepra-India, explained in his welcome address the aims and objectives of the project being launched in Hyderabad. Dr. Udaya Kiran, Senior Medical Officer, Lep-ra-Hyderabad project, proposed the vote of thanks.
Dr. Sree Krishna, Additional Director for Leprosy; the special Leprosy Officer, Dr. Jeelani; the training officer, Dr. Gurunath Babu; the zonal leprosy officers, and medical officers of the leprosy field attended.
While in India for the launch of Lepra-India in August, Lepra-U.K. Chairman Bill Peters, accompanied by Head of Programs and Projects Frank Black, inaugurated a new multidrug therapy program in Medak District, A.P. The district has a population of about two million with a very high leprosy prevalence of 9 per 1000, with 16,000 patients currently registered. Patients in Medak have previously only had access to the less-effective monotherapy (treatment with a single drug, dapsone). Now, through Lepra-India, four new leprosy control units and an urban leprosy program will get drugs, transport and running costs totalling Rs. 10 lakhs this year, with further support guaranteed for the next 3 years.
In addition to these operational programs, Lepra-India also allocates funds to other Indian organizations engaged in the fight against leprosy. Gramanava Nirman Samithi (GNNS) will receive the full operating costs this year for its screening and treatment program in the city of Hyderabad. The Gandhi Memorial Leprosy Foundation (GMLF) is another recipient of Lepra funds for its work in Calcutta, as is the Hoina New Life Trust in Koraput, Orissa.
Outside of India, much of Lepra's work since 1964 has been concentrated on a nationwide control program in Malawi, central southern Africa. There, in cooperation with the Malawian health services, the caseload has been dramatically reduced from almost 50,000 registered leprosy patients to just 2000. Much of the success of the program can be attributed to the introduction in 1983 of multidrug therapy to replace the former treatment with a single drug. Since 1980, Lepra has also implemented a comprehensive leprosy evaluation project in Malawi. This extensive population survey was established in the north of the country to identify who is most at risk from leprosy and should provide invaluable information to help understand the disease better. In 1986, a vaccine trial, which could lead to an immunization program providing permanent protection from leprosy, was incorporated into the evaluation project, under the auspices of WHO.
In South America, other programs benefitting from Lepra funding are an assessment of the extent of leprosy carried out by rural health workers in Peru and a pilot project for leprosy control units in the 26 districts of Brazil.
In addition to its field programs, a proportion of Lepra's Rs. six crores annual income is spent on research programs in Britain, seeking more effective early diagnosis treatment and prevention of leprosy. It also involves work on a potential vaccine and research aimed at discovering more about the leprosy bacillus, how it causes nerve damage, and why only a small proportion of those exposed to the disease actually develop it.
Lepra also funds a scientific Journal "Leprosy Review" and encourages future generations of leprosy researchers and medical staff by supporting short periods of leprosy study abroad for up to 20 medical students each year.
Perhaps the major problem Lepra faces in its fund raising and information work in Britain is the need to convince the public that leprosy still exists. Most of Europe has been free of endemic leprosy for almost 200 years, and many people in Britain now view it as an historical "biblical" disease. With an estimated 12 million people still suffering the ravages of leprosy-and the social ostracism which frequently results -a strong education program is vital to the mobilization of the essential support required if leprosy is really to be eradicated. -Kusht Vinashak 11 (1989) 12-16.
MLSM Anti-Leprosy Week Celebration, 1990. Maharastra Lokahita Seva Mandal (MLSM), a nonsectarian voluntary organization, has been engaged in antileprosy activities in H Ward East and P Ward of the Bombay Municipal Corporation since 1976. It covers a population of over 1.6 million through its SET program. Although health education is its routine activity, a special emphasis is made every year during Anti-leprosy Week.
The main feature of this year's Antilepro-sy Week celebration was in cooperation with the Western Railway-Bombay Division. To mark the inauguration of the week's celebration, a special local train, with a message exclusively on leprosy on 36 rack panels (usually used for commercial advertisements), was flagged off by Shri K. Subrah-manyan, General Manager, Western Railway, on the Bandra Station. This train, each compartment decorated with stickers and posters with leprosy awareness slogans, ran its routine schedule between Churchgate and Virar Station (over 60 km), benefitting a large number of railway commuters every day. Illuminated boards with leprosy slogans were also displayed at railway stations.
This would not have been possible without the initiative of Dr. M. P. Garg, Medical Superintendent, Western Railway. His generous support and inspiration helped to make the program a great success.
MLSM also held leprosy check-up camps and several exhibitions on local railway stations in the project area. Exhibitions were aided with audio-visual programs. Special lectures with slide shows were conducted for the nurses of S.N.D.T. college, and a similar program was organized at a training center of the Bank of India for their officers.
MLSM has put up four billboards at very prominent public places which will remain for the complete calendar year. In addition, several banners and posters were put up at public places. Ballpoint pens and metal key chains carrying leprosy messages and slogans were widely distributed. Leprosy transparencies were supplied to cinema halls for regular projection. Leprosy slogans were printed on BEST (city bus service) bus tickets; a total of 16 lakhs of such tickets are in circulation.
The public response was very encouraging. A good number of doubtful cases voluntarily came forward for diagnosis/confirmation right on the exhibition spot, and a few turned out to be with Hansen's disease. Similarly, a very large number of general skin cases along with a few Hansen's cases are received in our field office clinic regularly.
We now believe that although regular health education in our SET program is a must, the impact of this intensive and exclusive leprosy propaganda during Antilep-rosy Week is very impressive, positive and hence influential. -Mr. Jayadas, Program Director, MLSM.
NASEOH celebrates 30th World Day of the Disabled, 1990, and presents awards. On 19 March 1990, the National Society for Equal Opportunity for the Handicapped, India, (NASEOH), held an observation of the 30th World Day of the Disabled, 1990, in Bombay. During the celebration, the Shri B. J. Modi Foundation Award was presented to Dr. Bimalendu Narayan Roy, Dr. R. Ganapati was awarded the Late Shri N. D, Diwan Memorial Award, and awards were given to outstanding disabled employees, the self-employed, and employers of the disabled. Shri C. Subramaniam, Governor of Maharashtra, was the Chief Guest, and the Guest of Honor was Smt. Shakunthala Subramaniam.- From the Invitation.
Poona District Leprosy Committee Annual Report, 1988-1989. The Poona District Leprosy Committee (PDLC), whose Hon. President is Dr. Jal Mehta, conducts the following main projects: Dr. Bandora-walla Leprosy Hospital, Kondhawa Poultry and Dairy Farm, Common Vocational Training Project for the Handicapped, Dr. Minoo Mehta Industrial Production Co-operative Society, PDLC's Firodiya Rehabilitation Centre, and Urban Leprosy Control Projects for Pune and Solapur.
The Poona District Leprosy Committee, its Dr. Bandorawalla Leprosy Hospital, and several other projects continued to serve the cause of leprosy treatment and rehabilitation. The Dr. Minoo Mehta Industrial Production Co-operative Society for the Welfare of the Handicapped Ltd. has performed well, and the credit goes to the members for working hard in their own interests. A number of newly cured leprosy patients were placed in the Workshop of the Society for training and practical experience in various engineering jobs. Gradually, these trainees will be absorbed into other units, and another group of the handicapped will be taken for vocational training, thus keeping in motion the cycle of rehabilitation.
Sports activities involving the general community were further continued, leading to a healthy mingling of noninfectious leprosy patients and healthy persons, and thereby helping to lessen the leprosy stigma. This year emphasis was on health education, public awareness campaign, and rehabilitation of cured leprosy patients. The rest of the activities of treatment, control, and clinical research continued as before. We are beholden to the leprosy patients, the public, the Government and its various departments, the German Leprosy Relief Association, ICCO, NORAD, SIDA, Lions, Manos Unidas, CRS, TELCO, and others.-Dr. Jal Mehta, Hon. President.
Italy. ILEP personality moves to WHO. Dr. Enrico Pupulin, President of the As-sociazione Italiana Amici di Raoul Foller-eau (AIFO) and past president of ILEP (1982-1984), is to be chief of the WHO Rehabilitation Unit. On 1 May 1990 he succeeds Dr. Helander, who has retired, in this crucial post for the development of rehabilitation services worldwide. He is expected to continue the Unit's community-based rehabilitation approach.
Dr. Pupulin is currently responsible among other things for child rehabilitation services in the Castelfranco area of northern Italy. His interests in rehabilitation are also reflected in the policies of AIFO which has recently set aside about $0.9 million for projects in this field. For the time being he expects to continue as President of AIFO. - ilep FLASH 2 (1990) 1.
Kenya. A History of Leprosy in Tanzania. A pamphlet by Knud Balslev entitled "A History of Leprosy in Tanzania" is available from: African Medical and Research Foundation, Wilson Airport, P.O. Box 30125, Nairobi, Kenya. This valuable pamphlet describes the history of antileprosy work in Tanzania up to 1977. It thus provides the background to the present national program. There are chapters on the periods of both German and British colonial control. Of particular interest is the way it describes cooperation between government and voluntary agencies, the creation of a mechanism for that co-operation-the Tanzania Leprosy Association-and the planning for what today is one of the best examples of a real attempt at nationwide control of leprosy.
Another theme illustrated is the explosion in numbers of registered patients in the 1960s and 1970s as effective treatment was perceived as being available.
For friends of ILEP, the story is full of familiar faces: Dr. Anten, whose mother's fundraising efforts led to the creation of NSL; Dr. Felton Ross, now chair of our medical commission, whose visit in 1967 was a stimulus to training local doctors and supervisors; Dr. Robert Cochrane, who, as medical secretary of LEPRA, visited in 1930 and 1952; and above all, Dr. Harold Wheate, later secretary of our medical commission, who played a big role in Tanzania from 1954 to 1972.-ilep FLASH 1 (1990) 3.
Malawi. Karonga research progress. Last September the mammoth task of vaccinating 120,000 people out of a population of 140,000 in the Karonga District of Northern Malawi was completed after almost 4 years of work. This is the first stage in the trial of possible vaccination strategies against leprosy. Over the next 10 years as the population continues to be studied with exceptional care, we will see whether the vaccines used have any appreciable effect on the incidence of leprosy. The research population splits about equally into those who had previously had a BCG vaccination and those who had not. Different sub-cohorts have received either a supplementary BCG injection, an initial BCG, or a mixture of BCG and killed M. leprae in one of two different strengths.
The vaccination program was combined with the second total population survey of the Lepra Evaluation Project. During the next year statistical analysis will begin, comparing the latest survey results with data from the initial survey undertaken in the early 1980s. The initial priorities for analysis are leprosy incidence, the effectiveness of BCG against TB in this particular population, and any links with HIV. Many other issues will eventually be touched on in the scientific papers expected to result from the project.
Staff from the vaccination and survey program will be needed again for the third survey due to begin in 1992. In the meantime they are being used in an interesting new initiative. They are situated at local health clinics, seeing every new patient coming to the clinic, screening them for leprosy and skin conditions, and providing a testing service for TB and HIV. Apart from being a useful service to the community, it should help to ensure that new cases of leprosy in the vaccinated population are identified. In particular, it will test whether virtually every individual in the population comes to a health clinic at some time, and thus whether this could be a more cost- and time-effective method of undertaking total population surveys. Already in the first two months, over 16,000 people had been seen.-ilep FLASH 2 (1990) 1.
Mexico. Mexican MDT program. An agreement has been signed between the government of Mexico, the American Leprosy Missions and the Pan American Health Organization/WHO to set up a MDT program for the country. The objectives of the new program include stopping transmission in the community, detecting cases early and treating them, and integrating leprosy control into the general health service. Initially the program will be introduced into 10 Mexican states which contain about 21 million people -a quarter of the population. It is estimated that about 80% of the 17,000 registered leprosy patients in Mexico live in these states.
Most of the funding for the new program is being provided by the American Leprosy Missions. First year costs, including those of training 158 first-level personnel, are expected to be in the region of $23,500. Drugs for the program will be donated by the Sa-sakawa Memorial Health Foundation of Japan.
The document setting out the terms of the agreement emphasizes that all patients with active disease should receive MDT therapy.
The ten states with the greatest prevalence are: Colima, Sinaloa, Nayarit, Guanajuato, Jalisco, Michoacan, Sonora, Quertaro, Morelos and Guerrero. -ilep FLASH 2 (1990) 2.
Nigeria. MDT program to be expanded. Members meeting at the ILEP working session in Jersey in December discussed the new national initiative in Nigeria and plans for expanding the use of MDT to the whole country. Current estimates suggest there are 160,000 cases of leprosy in Nigeria, making it the African country with the largest number of cases. Of a total of 22 states, nine are presently without any form of assistance. The Jersey meeting agreed to support the process of implementing MDT in all these states. Members reached a preliminary agreement on which organizations would support which states. Further negotiations with the Nigerian government will be coordinated by NSL which is acting as the liaison agent.-ilep FLASH 1 (1990) 1.
Spain. Government leprosy hospital at Trillo to close. The government leprosy hospital at Trillo, near Madrid, is due to be closed down at the beginning of this year and all its patients will be transferred to Fontilles, which will be then the last leprosy hospital in Spain. The Sanatorio San Francisco de Borja at Fontilles (SF) is ILEP's Spanish member. It is well known in the east of Spain and is hoping to expand its activities to the whole of the country as a first stage toward the formation of a truly national leprosy association. Last year SF also decided to change its constitution to allow it to attend to patients outside Spain.- ilep FLASH 2 (1990) 3.
Switzerland. FIELDLINCS coordination and technical support grants. Field Links for Intervention and Control Studies (FIELDLINCS) is a recently created program designed to promote high quality field research on the TDR diseases-malaria, schistosomiasis, filariasis, trypanosomiasis, leishmaniasis and leprosy. The three goals of FIELDLINCS are: 1) to provide training in epidemiology, entomology and social sciences for individuals conducting field research on intervention strategies, and implementing control programs; 2) to promote field research networks as mechanisms for training in project design, methodologies and techniques of field research, and for project-to-project linkage to reduce the isolation of investigators; and 3) to work in close collaboration with TDR's disease-specific components to provide input into the selection and utilization of epidemiological, social science, and entomological methods appropriate for the study of tropical diseases.
For more information, write: Dr. Jacqueline Cattani, FIELDLINCS Coordinator, TDR, World Health Organization, 1211 Geneva 27, Switzerland.
Multicenter field trial call for participants. The Scientific Working Group on the Chemotherapy of Leprosy (THELEP) is planning a multicenter field trial to evaluate a multidrug regimen which would include ofloxacin, a fluoroquinolone with demonstrable activity against Mycobacterium leprae. Requirements for center participation include: 1) a well-organized outpatient treatment facility capable of receiving at least 100 new, untreated, or minimally treated (up to 6 months with dapsone therapy) mul-tibacillary patients per year; 2) ability to follow up the patients regularly through a field organization; and 3) facilities to carry out routine biochemical and other tests to monitor for toxicity. Qualified centers interested in participating in this trial should send a letter of intent providing information on their qualifications and facilities to: Dr. S. K. Noordeen, Chief Medical Officer, Leprosy Division of Communicable Diseases, World Health Organization, 1211 Geneva 27, Switzerland.
TDR/WHO offers project development grants to LDC scientists. The WHO/World Bank/UNDP Special Programme for Research and Training in Tropical Diseases (TDR/WHO) has established a Project Development Grant mechanism which is intended to enhance the involvement of scientists from developing countries in research to develop improved methods of controlling major tropical diseases. Only national scientists of developing countries who wish to conduct research on one or more of the six TDR/WHO tropical diseases (e.g., filari-asis, including onchocerciasis; leishmaniasis; leprosy; malaria; schistosomiasis; and African or American trypanosomiasis) arc eligible for these awards.
The Project Development Grants program is designed to provide catalytic support to assist in the formulation of technically sound proposals suitable for submission to the various TRD/WHO Steering Committees for more substantial funding. The maximum amount allowable per investigator under this nonrenewable grant is US$10,000. These funds may be used to seek the advice of recognized experts in the preparation of a research proposal, to gather baseline or other preparatory data, and/or to initiate a pilot project.
The application should be submitted on the official TDR/WHO "Director's Initiative Fund" application form. Potential applicants are encouraged to seek additional information from TDR/WHO Secretariats responsible for individual diseases. For application forms or to submit completed proposals, contact: Office of the Director, TDR, World Health Organization, 1211 Geneva 27, Switzerland.
U.K. Dr. Grace Warren retires. Dr. Grace Warren retired last year after 30 years of service for The Leprosy Mission. Her energetic and far-reaching ministry has received much acclaim; honors including the Order of Australia and Fellowship of both the Australian and Royal College of Surgeons (England), and the Taiwan Department of Health's Medal of Honor. -New Day Spring (1990) p. 17.
ILEP former President Farine retires. Marcel Farine, first President of ILEP and founding president of ALES, has retired. He has had a long and distinguished career in work on leprosy, particularly the social aspects of the disease.
In 1965-1966 he was a member of the group which met to discuss the formation of an international anti-leprosy organization. In September 1966 he presided over the constituent assembly of ELEP (ILEP's European forerunner), held in Berne. He became President again in 1973-1974.
Throughout the 1970s he kept up his work, speaking and researching on the human aspects in the treatment of leprosy in many different countries throughout the world.
In 1986 he played an important role in forming an ILEP working group to revise the statutes and internal rules of the organization. These were adopted at the working session in Malta in December 1987.
Hermann Kober, ILEP President, speaking at the dinner at the working session in Jersey in December, paid tribute to Marcel Farine. "He was the first President of the European federation, ELEP, and he led one of the most important Working Groups of ILEP which produced a manual on the social aspects of leprosy.
"We also thank Marcel Farine, however, for the fundamental contribution -reflecting his intelligence and sense of logic -to our constitution and bylaws, which arc the foundations of our cooperation. His constructive criticisms in discussion have always illuminated our thinking and improved our work together.
"It is with sadness, but also with great respect and deep gratitude that we say farewell to him today. We very much hope that we will still be able to call on him in the future. We know that mankind and, above all, those in need are always the first concern for our friend Marcel Farine." -ilep FLASH 1 (1990) 1.
Leprosy in Childhood. A revised edition of Leprosy in Childhood by Colin Mc-Dougall and Felicity Savage is available from TALC, P.O. Box 49, St Albans, Herts, AL1 4AX, England.
This set of color transparencies and written text has been fully revised and brought up to date and now includes a section describing the regimens of multiple drug therapy recommended for all cases by the WHO in 1982. It is intended as a general introduction to leprosy and is suitable for all health workers in areas where leprosy is endemic.
The set of 24 slides covers definition, prevalence, clinical types of leprosy, transmission, natural history of the disease, nerve damage, classification, foot ulcers, differential diagnosis, reactions, prevention and multiple drug therapy.
Cost of transparencies for self-mounting, with text: £3.50 (£2.75 to developing countries). Cost of mounted slides in plastic folder, with text: £4.90 (£4.40 to developing countries).-ilep FLASH 1 (1990) 3.
Rev. Silvano Perotti retires. Rev. Silvano Perotti, BD, former Director of The Leprosy Mission (TLM) Europe and latterly Deputy International Director and Director of Support and Development for TLM International, has retired after 15 years. Rev. Perotti has seen considered growth in the support of the TLM and will be greatly missed for his spiritual input and lively personality.-New Day Spring (1990) p. 17.
TAMILEP offers paperback edition of "Leprosy" to Third World countries. A paperback edition of the textbook entitled "Leprosy" (R. C. Hastings, ed.) is now available at the greatly reduced price of £4.00 per copy + packing and postage. This price is available to Third World countries only. The contents and quality of the paper arc the same as the first edition (1985) which was priced at £55.00. Copies may be ordered from: Teaching and Learning Materials, The Leprosy Mission International, 80 Windmill Road, Brentford, Middlesex TW8 0QH, U.K.
Orders from India should be sent to: D.A.H.W., 4 Gajapathy Street, Shenonagar, Madras 600 030, South India -Materials from Jane Neville, TLM.
U.S.A. ILA Congress. The International Leprosy Association has now fixed the dates of the next Congress which is to be held in Orlando, Florida, U.S.A., between 26 August and 7 September 1993. -ilep FLASH 2 (1990) 1.
New address for American Leprosy Missions (ALM). Effective 15 September 1990, the new address for ALM is: ALM International, 1 ALM Way, Greenville, South Carolina 29601, U.S.A. Toll free phone number is: 1-800-543-3131.
Zimbabwe. Leprosy in Zimbabwe ending. Associazione Italiana Amici di Raoul Fol-lereau (AIFO), the 1LEP coordinator for Zimbabwe, reports that the leprosy problem in the country is close to an end. The incidence of new cases is down to about 140 per annum in a population of 9 million, and about a third of those are among the refugees from Mozambique. A major concern now is to ensure that new cases continue to be recognized by general health staff. There is also suspicion of a link between AIDS and leprosy. Thus, new cases who present with leprosy in a manner unusual for the area -an advanced state or young age -are being routinely tested for HIV. - ilep FLASH 2 (1990) 3.
We were deeply saddened to learn of the death of Dr. John H. Hanks at his home in Baltimore, Maryland, U.S.A., on 11 July 1990. Dr. Hanks was an Honorary Vice President of the International Leprosy Association, and well known to generations of lep-rologists.