- Volume 58 , Number 1
- Page: 115–6
Cutaneous lymphoma masquerading as lepromatous leprosy
This department is for the publication of informal communications that are of interest because they are informative and stimulating, and for the discussion of controversial matters. The mandate of this JOURNAL is to disseminate information relating to leprosy in particular and also other mycobacterial diseases. Dissident comment or interpretation on published research is of course valid, but personality attacks on individuals would seem unnecessary. Political comments, valid or not, also are unwelcome. They might result in interference with the distribution of the JOURNAL and thus interfere with its prime purpose.
To the Editor:
A 15-year-old boy presented with generalized pruritus with ichthyosis and hyperpigmentation of the skin of 10 years' duration and generalized infiltration of the skin with beaded thickening of the earlobes and superciliary madarosis (Fig. 1) of 6 months' duration. Other systems were clinically normal except for generalized lymphadenopathy and mild splenomegaly. A clinical diagnosis of lepromatous leprosy was made, but repeated slit-skin smears from the earlobes did not reveal any acid-fast bacilli. A blood test showed a total white blood cell count of 20,000/cmm. Examination of the bone marrow revealed diminished numbers of mature cells and the predominance of myelocytes and lymphoblasts. The diagnosis of cutaneous non-Hodgkin's lymphoma was confirmed by a skin biopsy which showed dense subepidermal infiltrations by sheets of hyperchromatic round cells with minimal cytoplasm (Fig. 2). A section of a lymph node showed a loss of normal architecture and its replacement by sheets of immature and atypical lymphocytes.

Fig. 1. Cutaneous lymphoma seen on ear.
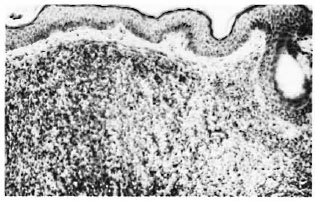
Fig. 2. Subepidermal monomorphous population of lymphoid cells (H&E × 125).
Non-Hodgkin's lymphomas are known to begin with skin lesions and remain localized to the skin for months or years before visceral involvement becomes evident (2). The specific cutaneous lesions are firm pink or red solitary nodules involving the skin of the head and neck region. Nonspecific skin lesions, like pruritus, generalized ichthyosis and hyperpigmentation as seen in our patient, are rare (3). Lepromatous leprosy may sometimes have to be differentiated from dermal leishmaniasis, nodular syphilides leukemia cutis, and histiocytic lymphoma (1). Malignant lymphomas constitute only 2.34% of all cancer cases in India (4). Our patient was misdiagnosed as lepromatous leprosy because of dense infiltrations of the face and earlobes.
-C. Balachandran, M.D.
Assistant Professor
Department of Dermatology and S.T.D.
-C . R. Srinivas, M.D.
Reader
Department of Dermatology and S.T.D.
-S . D. Senoy, M.D.
Assistant Professor
Department of Dermatology and S.T.D.
- K. Ramnarayan, M.D.
Professor
Department of Pathology
Kasturha Medical College and Hospital
Manipal 576119, India
REFERENCES
1. BALACHANDRAN, C, SRINIVAS, C. R., SINGH, K. K. and VENUGOPAL, N. Histiocytic lymphoma simulating lepromatous leprosy. Indian J. Lepr. 59(1987)332-333.
2. BRAVIRMAN, I. M. Lymphomas and allied disorders. In: Skin Signs of Systemic Disease. 2nd ed.Braverman, 1. M., ed. Philadelphia: W. B. SaundersCompany. 1981, pp. 109-173.
3. CHU, A. C. and EDELSON, R. L. Tumors of the lymphoreticular system. In: Dermatology. 2nd ed. Moschella, S. L. and Hurley, H. J., eds. Philadelphia: W. B. Saunders Company, 1985, pp. 1639-1671.
4. DESAI, P. B., MEHER-HOMJI, D. R. and PAYMASTER, J. C. Malignant lymphomas. A clinical study of 800 Indian patients. Cancer 18(1965)25-33.