- Volume 57 , Number 2
- Page: 476–82
Productivity loss due to deformity f rom leprosy in India1
ABSTRACT
The productivity loss in India due to deformity f rom leprosy was assessed in a random sample of 550 leprosy patients f rom a rural and an urban area in the state of Tamil Nadu. Logistic and log-linear regression analyses on these leprosy patients showed that elimination of deformity would: a) raise the probability of gainful employment f rom 42.2% to 77.6%; b) increase annual earnings per patient gainfully employed f rom Rs 2948 to Rs 6469; and c) raise overall earnings for all patients f rom Rs 1259 to Rs 5023 per year. The earnings of 550 control subjects (adult family members of the leprosy patients) were consistent with these predictions. Extrapolation to all of India's estimated 645,000 leprosy patients with deformity suggests that elimination of deformity would raise productivity by $130 million per year. The authors conclude that the development and evaluation of programs to eliminate deformity f rom leprosy deserve high priority.RÉSUMÉ
La perte de productivité qu'entraîne en Inde les invalidités dues à la lèpre a été évaluée dans un échantillonnage pris au hasard de 550 malades de la lèpre, provenant de régions rurales et urbaines dans l'état du Tamil Nadu. Des analyses de régressions logistique et linéaire logarithmique menées sur ces malades ont montré que l'élimination des invalidités entraînerait les résultats suivants: (a) elle augmenterait la probabilité d'un emploi rémunéré, de 42,2% à 77,6%; (b) elle accroîtrait les revenus annuels par malades rénumérés de 2948 roupies à 6469 roupies; (c) elle porterait les gains annuels globaux de 1259 roupies à 5023 roupies par an. Les revenus des 550 sujets-témoins (membres adultes de la famille des malades) correspondaient à ces prédictions. Une extrapolation de ces résultats à l'ensemble des 645.000 malades dont on estime qu'ils sont invalides en Inde, suggère que l'élimination des invalidités augmenterait la productivité de 130 millions de dollars par an. Les auteurs concluent que la mise en oeuvre et l'évaluation de programmes destinés à éliminer les invalidités dans la lèpre méritent une haute priorité.RESUMEN
Se calculó la pérdida de la productividad en la India debida a la deformidad causada por la lepra en base al estudio de una muestra al azar de 550 pacientes de una área rural y una urbana del estado de Tamil Nadu. Los análisis logisticos y de regresión log-lineal en estos pacientes llevaron a concluir que la eliminación de la deformidad: (a) podría elevar la probabilidad de empleo remunerado del 42.2 al 77.6%, (b) aumentaría el ingreso anual per capita de los pacientes de 1259 rupias a 5023 rupias. Los ingresos de 550 sujetos control (adultos convivientes de los pacientes con lepra) fueron consistentes con estas predicciones. Extrapolando estas consideraciones a los 645,000 pacientes con deformaciones estimados en la India, se calcula que la eliminación de la deformidad elevaría la productividad en 1 30 millones de dólares al año. Los autores concluyen que el desarrollo y la evaluación de un programa para eliminar la deformidad de la lepra es de alta prioridad.In 1985, there were 5.4 million registered leprosy cases worldwide (8). India, with 3.2 million of these cases (Report of the Working Group on the Eradication of Leprosy, 1982; Leprosy: status report for 1985-1986, 1986; Ministry of Health and Family Welfare, Government of India), has more reported cases than all other countries combined. The deformity, disability and stigma to leprosy patients, as well as the risk to the billions of persons living in areas where the disease is endemic, make it a disease of enormous proportion worldwide, but particularly in India. Yet policy makers must allocate scarce resources for control and treatment of disease between leprosy and other conditions. Since estimates of economic loss provide a valuable guide in these allocations (Andreano, R. and Helminiak, T. Economics, health and tropical diseases. Paper presented at a meeting on the Economics of Tropical Diseases, School of Economics, University of the Philippines, Manila, Philippines, 2-5 September 1986), this paper assesses the productivity loss from deformity due to leprosy in India.
Quantifying the productivity loss is of special importance because recent multidrug regimens, which promise greater control of leprosy, require more costly drugs and more careful monitoring of patients than simpler regimens. In addition, physiotherapy has been highly effective in limiting deformity if administered early (6), but substantial resources would be required to make it available universally.
Among leprosy cases in India, approximately 20% of cases have some degree of deformity and disability (Report of the Working Group of the Eradication of Leprosy, 1982, Ministry of Health and Family Welfare, Government of India) as a result of nerve damage. The primary damage from Mycobacterium leprae is nerve damage and hence, loss of function of nerve fibers. Common effects of the disease include clawed hand and toes, loss or blurring of vision, nose drop and other forms of disfigurement, and loss of sensation. Secondary damage results from injury to an anesthetic and/or deformed limb.
In addition to suffering physical impairments, patients are stigmatized, particularly when they are deformed or disfigured. Both social stigma and physical deformity may limit or preclude a patient's ability to engage in productive economic activity (1)• As a result, earnings may be reduced or entirely eliminated.
METHODS AND DATA
Data collection. To examine the relationship between deformity and productivity loss, two random samples were constructed: a) 550 leprosy patients with some degree of deformity and b) 550 adult family members of these patients as control subjects. To derive the samples of leprosy patients, two areas within the state of Tamil Nadu with a high prevalence of leprosy were selected- the urban area of north Madras and the rural area of Cyeyyar district. Among India's 31 states and union territories, the state of Tamil Nadu reported the greatest number of registered cases (674,000 in 1984), or 1 out of every 6 cases in the country (Leprosy: National Leprosy Eradication Program, 1985, Leprosy Division, Director of Medical Services and Family Welfare, Government of Tamil Nadu, India). Registration cards of leprosy patients from clinics in these areas listed approximately 3250 patients from the urban area and 2250 patients from the rural area. The cards were scanned for mention or treatment of nerve damage as a proxy for deformity. As expected, such evidence was found in approximately 20% of the patients. Half of these presumably deformed patients were chosen at random and visited at home. These patients whose deformity was confirmed by observation during the personal visit constitute the study sample of leprosy patients-325 from the urban area and 225 from the rural area. The control sample consists of 550 adults chosen at random from among the 1075 adult family members of the leprosy patients.
To obtain data about these leprosy patients and their families, two male investigators with master's level training in economics and with previous survey experience were recruited. A physician experienced in treating leprosy patients trained them for 25 hours in the essentials of the disease. One of the investigators interviewed the sample patients and all their adult family members in Tamil, the regional language, between July 1985 and July 1986. The family interview totaled about three hours and covered the disease history of the patient and approximately 80 socioeconomic items about the patient and each adult family member. Whenever a respondent could not answer a question directly, the interviewer restructured it in a form consistent with available data. For example, if a respondent could not report his present age directly, it was derived from his age at marriage, the interval from marriage until the birth of his first child, and the current age of that child. The duration of deformity was derived similarly. Patients who gave false addresses to keep their illness secret were contacted at the clinic when they came for drugs. To assure complete and apparently reliable data, the interviewers requested meetings through friends and relatives, and returned to a subject's house as often as needed; the Tamil author (EM) personally attended one third of the interviews. He met privately with the 46 patients who initially declined to be interviewed. Eventually, every patient approached agreed to cooperate and responded to every question.
Physical impairments of the hands, feet, and eyes apparently due to leprosy were graded according to the deformity grading scale of the World Health Organization (12). For the hand, "0 " represents no impairment, "1 " insensitive hand, "2 " trophic ulcers and injuries and/or mobile claw hand and/or slight absorption, and "3 " denotes wrist drop or fingers clawed and joints stiff and/or severe absorption of fingers. For the foot, "0 " represents no impairment, "1 " insensitive foot, "2" trophic ulcers and/or clawed toes or foot drop and/or slight absorption, and "3 " contracture and/or severe absorption. For the eyes, "0 " represents no impairment, "1 " denotes redness of conjunctiva, "2 " denotes lagophthalmos and/ or blurring of vision and/or inflammation of the globe, and "3 " denotes severe loss of vision or blindness. The authors scaled facial disfigurement as "0 " representing no damage, "1 " representing slight facial disfigurement, and "2 " representing nose drop and/or severe disfigurement.
Assessment of productivity. A person's economic productivity, i.e., contribution to output of the economy, depends on earnings and the relationship between earnings and output. In this study, earnings are the sum of wages and salaries from manual labor and other forms of paid employment, profit from trade or business, and the individual's prorata share of the family's earnings from the family farm. Annual earnings were calculated by multiplying the number of days an individual reported working during the last year times the average earnings per day. An individual who had any earnings during the past year was termed "gainfully employed."
To calculate the economic loss from deformity, it was necessary to compare the average earnings of groups of leprosy patients under two alternative conditions: a) with their present levels of deformity, and b) if all deformities could have been completely eliminated. Expected annual earnings under each condition was estimated as the product of the proportion of the group gainfully employed times the average annual earnings of those gainfully employed.
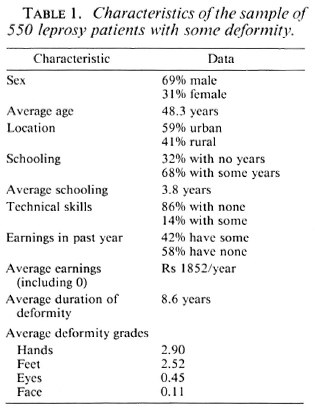
To estimate the proportion of a group gainfully employed, gainful employment was first analyzed by logistic regression on all 550 leprosy patients. The dependent variable, the presence of earnings, was coded as "1 " ifthe patient reported positive earnings (working at least one day per year with positive earnings), and "0" otherwise. The independent variables of greatest interest were the deformity grades. To improve the fit of the logistic regression, other major determinants of earnings were considered in the equation. These include sex, urban or rural location, presence of schooling, and presence of technical skills. Table 1 lists the variables considered relevant for examining the relationship between physical impairments and earnings, and presents their mean values and distributions for leprosy patients in the sample.
Next, the amount of annual earnings was examined for the 232 gainfully employed leprosy patients using multiple regression with a log-linear specification. That is, the dependent variable was the natural logarithm of earnings per year (in rupees) and independent variables were those in the logistic regression. This log-linear specification seemed most appropriate because the distribution of earnings was skewed to the right, and males and urban residents tended to earn several times as much as females and rural residents, respectively. Nevertheless, an ordinary linear specification was fit as a sensitivity analysis. Furthermore, to validate results derived from leprosy patients, projected earnings of leprosy patients without deformity were compared with actual earnings of control subjects. Finally, the regression equations were used to estimate what the leprosy patients' earnings would have been ifthey had been free of deformity.
RESULTS
Table 1 shows that males predominate the sample of leprosy patients, a finding consistent with other epidemiological studies of leprosy (12). Table 2 shows that the feet are the site most likely to be deformed; the face is least likely. The average grade of deformity in the limbs increased with the duration of deformity, reflecting the progressive nature of deformities in leprosy.
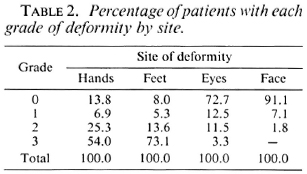
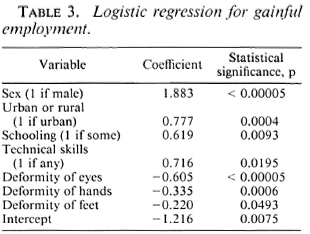
Table 3 reports the results of the logistic regression for gainful employment. All of the deformity variables are statistically significant and negative in sign, as expected. Due to minimal facial deformity, that variable was not statistically significant and was not included in the final specification. Age over 50 years was also tested and its coefficient was not significantly different from zero. Overall, 42.2% of the sample leprosy patients were gainfully employed.
To estimate the average annual earnings during the last year of all leprosy patients with deformity, the proportion of this population gainfully employed (42.2%) was multiplied times the geometric mean annual earnings of gainfully employed leprosy patients in the study (Rs 2948), giving Rs 1259 per year.
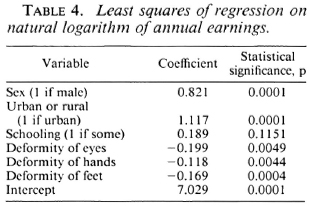
Table 4 shows the log-linear regression results for level of earnings. In general, the predictors of earnings per day acted in the same direction and with comparable levels of statistical significance as predictors of gainful employment. As the coefficient for "technical skills" was not statistically significant, that variable was eliminated from the model. The geometric mean of earnings, rather than the arithmetic mean, has been used unless indicated otherwise to be consistent with the use of log-linear regression.
To estimate average earnings if all deformity were eliminated, the proportion gainfully employed and their average earnings were estimated from the logistic and log-linear regression equations, respectively. To predict the effects of no deformity, first each of the independent variables for which disability was changed from its current level to zero (no deformity). Next, the coefficient of each of the three deformity variables (hands, feet, and eyes) was multiplied by the change in deformity level for that variable. The three resulting products were added. These changes raised the logistic score by 1.56 units, thereby increasing the probability of being gainfully employed from 42.2% with deformity to 77.6% with no deformity.
Similar calculations for level of earnings raised the natural logarithm of earnings by 0.774, thereby raising average earnings, given that one is gainfully employed, to Rs 6469. Together, these two estimates imply that eliminating deformity would raise the average earnings of a leprosy patient to Rs 5023 per year. Thus, the elimination of deformities would boost earnings to four times their present level of Rs 1259, an increase of Rs 3764. The sensitivity analysis used to examine the effect of alternative specifications estimated annual earnings per leprosy patient as a single linear equation of the same independent variables used in the two separate equations. That specification indicated that elimination of deformity would boost earnings by Rs 2418 per average leprosy patient per year.
The comparison of employment status and earnings of leprosy patients and control subjects in Table 5 reveals qualitatively similar patterns. Overall, only 42.2% of the leprosy patients were gainfully employed compared to 65.5% of controls. Male leprosy patients were 30% and female leprosy patients 61% less likely to be gainfully employed than controls. Leprosy patients earned 14% (male) to 38% (female) less per day worked than controls of the same sex. Among control subjects, males enjoyed a modest advantage over females in employment and earnings; among leprosy patients, males had a substantial advantage. Among persons gainfully employed, leprosy patients worked about the same number of days as control subjects.
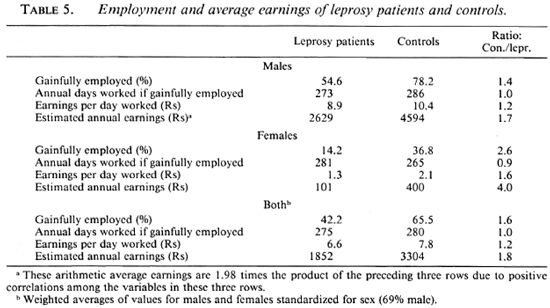
For comparison with the regression results, the arithmetic average earnings of leprosy patients in Table 5 is Rs 1852 per year and that of control patients is Rs 3304. As expected, the arithmetic average of leprosy patients is higher than the regression estimate based on the geometric mean. Earnings of control patients were 1.7 times those of leprosy patients for males, 4.0 times for females, and 1.8 times for both sexes combined.
Except for females, these relationships are smaller than the fourfold ratio from the regression results. Factors that could explain this finding include the following: earnings of control subjects were standardized only for sex, but not for location, schooling, and skills; stigma from leprosy might affect relatives of leprosy patients and depress their earnings; the need to care for a family member with leprosy may reduce the earnings of control subjects; patterns between arithmetic means may differ from those between geometric means.
The validity of these survey results and projections is supported by their consistency with patterns in the International Labor Office (ILO) data (4). ILO data for India for 1985 show that females had higher unemployment rates than males (51% vs 43%), and that females worked disproportionately in the two lowest wage industries (agriculture and services). The absolute rates in this study are not comparable with ILO data, however, because of numerous differences in definitions and scope of the data.
To extrapolate the regression results to a national level for India, it was noted that the country reported 3,225,302 registered leprosy cases in 1985. The number of leprosy patients with some deformity is estimated at 20% of this nuiVtber, or 645,000. Thus, the income gain from eliminating deformity in all registered deformed leprosy patients would be Rs 2.43 billion (645,000 times Rs 3764).
The gain in India's gross national product (GNP) is less than the income gain because of substantial unemployment and underemployment. The shadow wage rate to the market wage rate approximates the net increase in GNP from one unit of labor. Lal (7) estimated the ratio of shadow-to-markct wages for all urban areas in India as 0.62. For rural areas, where these ratios were derived by state (and reported only for males), the median value was 0.94. These ratios were weighted by the expected aggregate incomes of the 225 rural and 325 urban leprosy patients if their deformity were eliminated to yield a weighted average ratio of 0.66. Thus, the increase in India's GNP would be Rs 1.61 billion. At the 1985 exchange rate of US$1 equals Rs 12.33 (5), this amount is equivalent to about US$ 130 million.
DISCUSSION
As an indication of the magnitude of the $130 million gain to the Indian economy from eliminating deformity, this amount is one-eleventh of India's entire official development assistance for all purposes from all sources in 1985 ($ 1,470 million) (13). Our extrapolation to all of India provides an order-of-magnitude estimate of productivity losses from leprosy. If additional data were available, this estimate could be refined by including the following factors: a) Deformity due to unreported cases of leprosy.
Available data generally cover only patients who have been under treatment. Deformities and disabilities may progress beyond the completion of treatment, or in patients who were never registered, b) Losses from premature mortality, c) The national mix of leprosy patients between urban and rural areas. This analysis used the proportions in the sample (59% urban) and a conservative aggregation through geometric means, d) Current and potential earnings of leprosy patients in other parts of India. Although the prevalence of leprosy in Tamil Nadu is higher than in India as a whole, there was no reason to expect the distribution of severity not to be representative.
The productivity loss estimated in this study is termed an indirect cost of illness. The direct cost of an illness refers to the costs of medical care to control or treat the illness, whether paid by the patients or society. While direct costs have not been assessed systematically, Wardcker (11) found that the development of deformity is responsible for increased use of medical care. Thus, deformity in leprosy adds not only to indirect costs but to direct costs as well.
While the desirability of controlling deformity is undeniable, the epidemiology of deformity is not yet well understood. Some studies suggest that very regular attendance at clinics (3,10) and extended regular use of dapsone may be associated with increased deformity (2,9). The World Health Organization now recommends multidrug therapy (MDT) (which combines dapsone with bactericidal agents), but its long-term safety and efficacy has not as yet been thoroughly tested (12).
Srinivasan and Noordeen (10) indicated the need for a prospective longitudinal study of the epidemiology of deformity in leprosy. The substantial productivity loss calculated here underscores this need. The proposed study should compare a program of MDT, physiotherapy, and careful monitoring of patients to prevent deformity against conventional therapy. While such treatment protocols may be costly to implement, the results of this study suggest that failure to control deformity may be even more costly.
Acknowledgments. This work was supported in part by the University Grants Commission of India. American Leprosy Missions. Inc., the Damien Foundation (Belgium), and the Takemi Program. The authors thank J. Lee Margraves for his assistance in data analysis.
REFERENCES
1. BRAND, P. W. and FRITSCHI, E. P. Rehabilitation in leprosy. In: Leprosy. Hastings, R. C, ed. Edinburgh: Churchill Livingstone, 1985. pp. 287-319.
2. DANESHMEND, T. K. The neurotoxocity of dapsone. Adverse Drug React. Acute Poisoning Rev. 3(1984)43-58.
3. GUPTE, M. D. Dapsone treatment and deformities: a retrospective study. Lepr. India 51(1979)218-234.
4. INTERNATIONAL L ABOUR O FFICE. Year Hook of Labour Statistics 1987. Geneva: International Labour Office, 1987. pp. 330. 370, 570.
5. International statistics. Table 3.28 Foreign exchange rates. Fed. Reserve Bull. 72(1986)A68.
6. KELLY, E. D. Physical therapy in leprosy for "paramedicals." Bloomfield, New Jersey: American Leprosy Missions. 1981.
7. LAL, D. Prices for Planning; Towards the Reform of Indian Planning. London: Heinemann Educational Books Limited, 1980, pp. 173. 181.
8. NOORDEEN, S. K. and LOPEZ BRAVO. L. The world leprosy situation. World Health Stat. 39(1986)124.
9. RADHAKRISHNA. S. and NAIR, N. G. Association between regularity in dapsone (DDS) treatment and development of deformity. Int. J. Lepr. 55(1987)425-434.
10. SRINIVASAN, H. and NOORDEEN, S. K. Epidemiology of disability in leprosy. Int. J. Lepr. 34(1966)159-174.
11. WARDEKAR, R. V. Sulphone treatment and deformity in leprosy. Lepr. India 40(1968)161-171.
12. WHO STUDY GROUP. Epidemiology of leprosy in relation to control. Geneva: World Health Organization. 1985. Tech. Rep. Ser. 716.
13. WORLD BANK. World Development Report 1987. New York: Oxford University Press, 1987.
Ph.D., The Takemi Program in International Health and Department of Health Policy and Management. Harvard School of Public Health, and the Harvard Institute for International Development (HIID), Boston Massachusetts, U.S.A.
Reprint requests to: Dr. Shepard, HIID, One Eliot Street, Cambridge, Massachusetts 02138, U.S.A.
Received for publication on 21 March 1988.
Accepted for publication in revised form on 23 November 1988.
1. This paper was presented in part at the 116th Annual Meeting of the American Public Health Association, Boston, Massachusetts, U.S.A., 15 November 1988.