- Volume 67 , Number 1
- Page: 1–5
Role of S-100 staining in differentiating leprosy f rom other granulomatous diseases of the skin
ABSTRACT
Since Mycobacterium leprae are rarely demonstrable in the tuberculoid spectrum of leprosy, a confirmatory diagnosis of leprosy can be made on the basis of finding active destruction of cutaneous nerves by granulomatous inflammation in a skin biopsy. Immunoperoxidase staining for S-100 protein, which is a marker for Schwann cells, was used to delineate nerves in lesional skin biopsies of 25 patients with tuberculoid and borderline tuberculoid leprosy as well as 15 controls with nonleprous granulomatous inflammation. Four different patterns of nerve damage were observed: infiltrated, fragmented, absent, and intact. All of the non- leprous granulomatous dermatoses showed only intact nerves, either inside or outside the granuloma, and so S-100 staining can be used to rule out leprosy.RÉSUMÉ
Comme Mycobacterium leprae est rarement mise en évidence dans les formes tuberculoïdes da la lèpre, un diagnostic de certitude de la lèpre peut être effectué en se basant sur la trouvaille, dans une biopsie cutanée, de nerfs cutanés détruits par l'inflammation granulomateuse. Le marquage de la protéine S-100 par immunopéroxydase, qui est spécifique des cellules de Schwann, a été utilisée sur de biopsies cutanées pour souligner les nerfs dans les lésions de 25 patients atteints de lèpre tuberculoide et borderline tuberculoide ainsi que 15 contrôles présentant des inflammations granulomateuse non-lépreuses. Quatre aspects différents d'atteinte nerveuse ont été observés: infiltré, fragmenté, absent et intact. Toutes les lésions granulomatoses non-lépreuses ne montraient que des nerfs intacts, que ce soit à l'intérieur ou à l'extérieur du granulome, et donc l'immuno-marquage par la protéine S-100 peut être utilisé pour écarter la lèpre.RESUMEN
Debido a que Mycobacterium leprae es raramente demostrable en la lepra tuberculoide, el diagnóstico confirmatorio de la enfermedad puede hacerse si se examina la destrucción activa de los nervios cutâneos por la inflamación granulomatosa en una biopsia de piel. En el presente estúdio, la tinción immunoquímica con anticuerpos marcados con peroxidasa para la proteína S-100, la cual es un marcador de las células de Shwann, lue usada para delinear los nervios en las biopsias de piel lesional de 25 pacientes con lepra tuberculoide y tuberculoide subpolar, y en 15 controles con inflamación granulomatosa no leprosa. Se observaron 4 patrones diferentes de dano a nervios; infiltrados, fragmentados, ausentes e intactos. Todas las dermatosis granulo- matosas no leprosas mostraron sólo nervios intactos tanto dentro como lucra del granuloma. La tinción para S-100 pcude usarse para descartar la lepra.Leprosy is most easily diagnosed when Mycobacterium leprae are demonstrable in diseased tissues, but this is often difficult in the indeterminate and in the tuberculoid types of leprosy in which M. leprae are rarely detected. Histological evidence of active destruction of a cutaneous nerve by granulomatous inflammation is widely accepted as a feature of tuberculoid leprosy. However, identifying remnants of the nerve in the granuloma may be difficult in some instances, and morphologic similarities with granulomatous dermatoses, such as lupus vulgaris, secondary syphilis, sarcoidosis, etc., add to the problem.
S-100 protein is an immunocytochemical marker of Schwann cells of nerves which is also found in normal neural tissue (neurons and glial cells) melanocytes and Langerhans' cells of the skin, interdigitating reticulum cells of the lymph nodes, chondrocytes, myoepithelial cells and ducts of the sweat, salivary and mammary glands, serous glands of the lung, fetal neuroblasts and sustentacular cells of the adrenal medulla (10).
There are three reports in the literature which address the utility of the immunoperoxidase staining of S-100 protein in skin biopsies as an aid in the diagnosis of tuberculoid leprosy (5,9,16). Narayan, et al . (12) have found that S-100 is a sensitive and reliable marker of nerve damage.
The present study was undertaken to examine with S-100 staining the different patterns of cutaneous nerve involvement in the tuberculoid spectrum of leprosy and other granulomatous conditions of the skin; to correlate these with the clinical and histo- pathological findings and also to determine whether S-100 staining will demonstrate fragmented, infiltrated, or the absence of dermal nerves.
MATERIALS AND METHODS
Twenty-five consecutive patients with a clinical diagnosis of tuberculoid leprosy (TTHD; N = 9) and borderline tuberculoid leprosy (BTHD; N = 16), according to the Job and Chacko classification (8), who attended the Dermatology Department of Christian Medical College Hospital, Vellore, India, in 1995 and 1996 were included in the study. These patients had cutaneous anesthetic hypopigmented or erythematous macules or plaques and did not have acid- fast bacilli (AFB) in their slit-skin smears; eight of them were in type 1 reaction. Patients who had received prior antileprosy treatment for more than 3 months and whose skin biopsies were reported as indeterminate leprosy were excluded from the study. Skin biopsies from representative lesions were examined histologically using hematoxylin and eosin (H&E) staining and a modified Fite-Faraco technique for M. leprae . These lesions were reported as either tuberculoid leprosy (N = 11 ) or borderline tuberculoid leprosy (N = 14). The clinical and histopathological findings, including the presence of AFB, were noted.
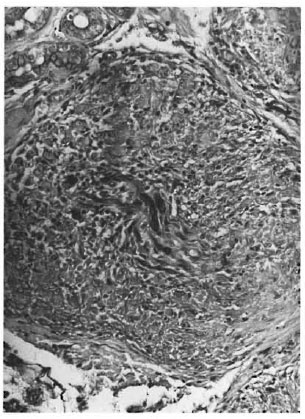
Fig. 1. Fragmented nerves inside a granuloma detected by S-100 protein (avidin-biotin peroxidase complex x200).
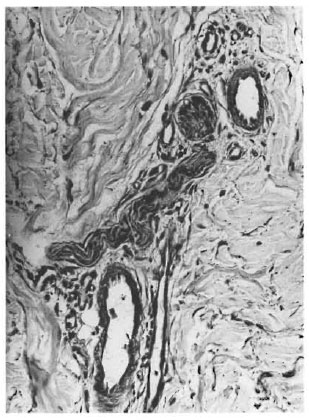
Fig. 2. Intact cutaneous nerve detected by S-100 protein (avidin-biotin peroxidase complex x200).
Fifteen consecutive patients with a clinical and/or histological diagnosis of granulomatous dermatosis other than leprosy (9 cases of tuberculosis of the skin, 1 case of sarcoidosis and 5 cases of granulomatous inflammation of unknown cause) were included as controls.
The 40 skin-biopsy specimens were subjected to S-100 immunoperoxidase staining (9) in two batches of 20 each. The S-100- stained slides were read without any reference to the clinical data.
The clinical diagnoses, histopathological features and S-100 staining patterns were then correlated. Diagnostic efficacy of the test in terms of specificity and sensitivity were calculated (by using 2x2 tables) using clinico-histopathological features as the "gold standard." Correlation between the presence of AFB in tissue sections and the pattern of neuritis by S-100 staining and the agreement between the clinical and histological diagnoses were also analyzed.
RESULTS
Four different patterns of nerve involvement were noted by S-100 immunoperoxidase staining: a) Infiltrated: dark staining, fibrillar structures in a wavy pattern associated with inflammatory cells; b) Fragmented: small, dark staining, fibrillar structures, usually multiple, inside a granuloma (Fig. 1); c) Absent: no dark staining fibrillar structures in or outside the granuloma; and d) Intact: dark staining, large fibrillar structures in a wavy pattern with no inflammatory cells inside (Fig. 2). These were seen in and outside the granulomas. Figure 3 shows the percentage distribution of the four patterns. Table 1 shows the correlation between the pattern of nerve involvement by H&E staining and S-100 staining.
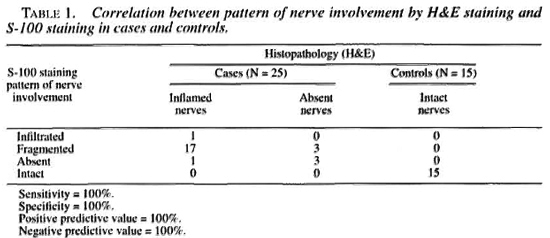
By S-100 immunoperoxidase staining, the skin biopsies with tuberculoid leprosy (TTHD) showed only fragmented nerves (100%); whereas those with borderline tuberculoid leprosy (BTHD) showed infiltrated (7.2%), fragmented (64.2%) and absent nerves (28.6%). Intact nerves were not present in these leprosy biopsies. Skin biopsies from the 15 controls contained intact nerves only. Nine of 14 BTHD and all of the 11 TTHD biopsies showed the fragmented nerve pattern. Thus, there was a more significant probability of finding a fragmented nerve pattern in TTHD than in BTHD patients (Fischer's exact text, p = 0.04).
Of the 8 cases which clinically showed features of type 1 reaction, 5 had fragmented nerves and 3 showed an absence of nerves in S-100-stained sections. There was no significant correlation between the morphological type of skin lesions or the sensory impairment of the skin lesion and the S-100 staining pattern.
The agreement between the clinical and histological diagnoses of leprosy cases was 84% (kappa = 0.66) (Table 2).
The presence of AFB in a skin-biopsy specimen did not significantly affect the pattern of cutaneous nerve destruction.
Of the four cases which did not show nerves by S-100 staining, three (75%) were clinically in type 1 reaction.
DISCUSSION
The fragmented pattern of nerve damage due to dermal neuritis was the most common pattern seen in the 25 leprosy cases and was more often seen in tuberculoid leprosy than in borderline tuberculoid leprosy. Intact nerves were not observed in any of the leprosy cases. This may be due to the immunity of the patient mounting a nerve destructive inflammatory response, forming granulomas. The 15 controls, however, showed intact nerves either inside or outside the granuloma. This enabled exclusion of leprosy in the controls, including those who were reported as having a granulomatous inflammation of unknown causes.
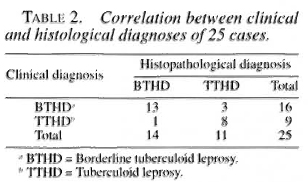
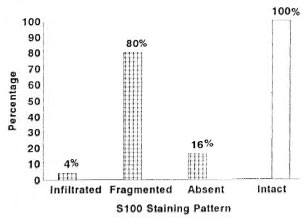
Fig. 3. Histogram showing the distribution of S-100 staining patterns of cutaneous nerve involvement;  = leprosy case;
= leprosy case;  = control.
= control.
By statistical analysis, it was found that S-100 staining was as good as H&E staining for the diagnosis of tuberculoid forms of leprosy. It was, however, superior to H&E staining in identifying the destruction of dermal nerves in leprosy. Fleury and Bacchi (5) in their study found that 8 out of 9 biopsies with a clinical diagnosis of tuberculoid leprosy, but with no histological or bacteriological evidence of the same, showed cutaneous nerve alteration by S-100 staining. They concluded that the use of S-100 staining to visualize remnants of peripheral nerves represents an efficient auxiliary aid in the diagnosis of leprosy. In a study by Job, et al . (7) out of 20 skin biopsies with clinical suspicion of tuberculoid leprosy, histologically reported as granulomatous inflammation, 14 showed nerve fragments in the granulomas, enabling a definite diagnosis of tuberculoid leprosy. Singh, et al . (16) concluded that the complete absence of nerve twigs, either inside or outside the granuloma, is the most reliable criterion for the diagnosis of tuberculoid leprosy. In contrast, in our series of 25 cases 80% showed fragmented nerves, while only 16% did not have demonstrable nerves. The present study clearly confirms the observation of earlier workers that the disorganization and destruction of dermal nerves is a far more consistent and frequent finding (84%) than the absence of nerves (16%) in the diagnosis of tuberculoid disease.
While agreement of clinical and histological diagnoses in earlier studies showed an average agreement of 50% (3, 15) in the present study it was 84%. Disagreement centered upon a) the absence of AFB and b) nerve-related histopathology.
In this study, 36% (9/25) of the skin-smear-negative leprosy cases showed AFB in tissue sections in the dermal nerves in 7 and in the granulomas in 2. This was consistent with the finding of Fleury and Aranda (4). However, in a recent study by Ponnighaus, et al . (13) there were AFB in the skin sections in 3.3% and in the nerve biopsies in 36.3% of the patients. The presence of AFB in the dermal nerves or granulomas did not have a significant effect on the pattern of nerve destruction.
With the World Health Organization's goal of reducing the prevalence of leprosy to 1 per 10,000 population by the year 2000 (17), as the incidence of leprosy declines, the expertise to diagnose leprosy may also be expected to decrease and S-100 immunoperoxidase staining could prove to be an effective aid in the diagnosis and study of patterns of cutaneous nerve involvement in the tuberculoid forms of leprosy.
REFERENCES
1. Boni, R., Burg, G., Docínoghu, A., Ilg, E. C., Schafer, B. W., Muller, B. and Heizmann, C. W. Immunohistochemical localization of the Ca2+ binding S-100 proteins in normal human skin and melanocytic lesion. Br. J. Dermatol. 137(1997)39-43.
2. Calissano, P., Moore, B. W. and Friesen, A. Effect of calcium on S-100, a protein of the nervous system. Biochemistry 8(1969) 4318-4326.
3. Fine, P. E. M., Jon, C. K., Lucas, S. B., Meyers, W. M., Ponnighaus, J. M. and Sterne, J. A. C. Extent, origin and implication of interobserver variation in the histopathological diagnosis of suspected leprosy. Int. J. Lepr. 61(1993)270-282.
4. Fluery, R. N. and Aranda, C. M. Detection of AFB in tuberculoid biopsies. (Letter) Int. J. Lepr. 63(1995)103.
5. Fleury, R. N. and Bacchi, C. E. S-100 protein and immunoperoxidase technique as an aid in the histopathologic diagnosis of leprosy. Int. J. Lepr. 55(1987)338-344.
6. Jacob, M., Chacko, C. J. G., Arunthathi, S. and Chandi, S. M. Significance and interpretation of nerve changes in skin biopsies when present in association with common dermatological conditions. (Abstract) Int. J. Lepr. 52 Suppl.(1984)755.
7. Job, C. K. Nerve damage in leprosy. (XIII Leprosy Congress State of the Art Lecture) Int. J. Lepr. 57(1989)532-539.
8. Job, C. K. and Chacko, C. J. G. A simplified six group classification of leprosy. Lepr. India 54(1981)14-16.
9. Job, C. K., Drain, V., Df.ming, A. T., Hastings, R. C. and Gerber, M. A. Role of S-100 protein as a marker for Schwann cells in the diagnosis of tuberculoid leprosy. (Letter) Int. J. Lepr. 58(1990)392-393.
10. Khan, H. J., Marks, A., Tiiom, H. R. T. and Baumai, R. Role of antibody to S-100 protein in diagnostic pathology. Am. J. Clin. Pathol. 79(1983)341-347.
11. Moore, B.W. A soluble protein, characteristic of the nervous system. Biochem. Biophys. Res. Commun. 19(1965)739-744.
12. Narayan, R., Maiieswari, P. K. and Desikan, K. V. Detection of S-100 protein and antieeramide antibodies in leprosy patients by ELISA. Lepr. Rev. 68(1997)117-124.
13. Ponnighaus, J. M., Leinhardt, C., Lucas, S., Fine, P. E. M. and Sterne, J. A. C. Comparison of bacillary indexes in slit skin smears, skin and nerve biopsies; a study from Malawi. Int. J. Lepr. 65(1997)211-216.
14. Schafer, B. W. and Heizmann, C. W. The S-100 family of EF-hand calcium binding proteins functions and pathology. Trends Biochem. Sci. 21(1996)134-140.
15. Sehgal, V. N., Rege, V. L. and Rey, M. Correlation between clinical and histopathological classification of leprosy. Int. J. Lepr. 45(1977)278-280.
16. Singh, N., Akora, V. K., Ramam, M., Tickoo, S. K. and Bhatia, A. An evaluation of the S-100 stain in the histological diagnosis of tuberculoid leprosy and other granulomatous dermatoses. Int. J. Lepr. 62(1994)263-267.
17. WORLD HEALTH ORGANIZATION. Action Programme for the Elimination of Leprosy. Status Report. Geneva: World Health Organization, 1996.
1. MD.; Department of Dermatology.
2. M.N.A.M.S.; Department of Dermatology.
3. M.D.. Dip. N.B.F.; Department of Dermatology.
4. M.D.. Department of Dermatology.
5. M.D.. Ph.D.. F.I.C.(Path.), Department of Pathology.
6. M.Sc., Ph.D., Department of Biostatistics, Christian Medical College and Hospital, Vellore 632 004, N. A. District, Tamil Nadu, India.
7. M.D., St. Thomas Hospital and Leprosy Center, Chettupattu 606 801. T. S. District, Tamil Nadu, India.
8. St. Thomas Hospital and Leprosy Center, Chettupattu 606 801. T. S. District, Tamil Nadu, India.
Reprint requests to Professor George at the above address or FAX 91-416-32035; e-mail: abraham@cmc.ernet.in
Received for publication on 9 July 1998.
Accepted for publication in revised form on 15 December 1998.