- Volume 67 , Number 1
- Page: 13–8
Cluster of leprosy cases in Kona, Hawaii; impact of the compact of free association
ABSTRACT
International travel and migration will continue to contribute to the changing patterns of Hansen's disease (HD) in the United States. The majority of cases will be immigrants and refugees entering the country f rom leprosy-endemic regions. The Compact of Free Association, through its provision of free travel between the Freely Associated States and the United States without need for health screening, has created new public health issues. This cluster of HD cases in Kona, Hawaii, U.S.A., highlights the difficulties in detecting and monitoring the spread of disease in immigrant populations. This is a growing problem only likely to worsen in the coming years. In groups with cultural, language or other socioeconomic barriers, special and creative methods may be needed to tackle the problems of detection, treatment and education. Clinicians must remain mindful of the diagnosis of HD in high-risk groups.RÉSUMÉ
Les voyages internationaux et les migrations vont continuer à façonner les aspects variables de la maladie de Hanson (MH) aux Etats Unis. La majorité des cas seront des immigrants et des réfugiés qui entrent dans le pays en provenance de régions où la lèpre est endémiques. La "Compact of Free Association", grâce aux voyages gratuits qu'elle distribue entre les Etats Librement Associés et les Etats Unis, sans l'obligation de visite médicale, a créé de nouveaux problèmes de santé publique. Un foyer de cas de MH à Kona, Hawaï, Etats-Unis, met en lumière les difficultés que l'on peut recontrer à détecter et contrôler la transmission de maladies dans les populations immigrantes. Ceci est un problême de plus en plus important qui pourrait bien empirer dans les prochaines années, parmi les groupes présentant dos différences culturelles, linguistiques et socio-éconimiques importantes, dos méthodes particuliàres et créatives seront probablement requises pour appréhender les problèmes de détection, de traitement et d'éducation. Les cliniciens doivent rester vigilants afin de diagnostiquer la MH parmi les groupes à haut risque.RESUMEN
Los viajes internacionales y la migración seguirán modificando los patronos de incidência de la enfermedad de Hansen (HD) en los Estados Unidos. La mayoría de los casos nuevos serán inmigrantcs y refugiados de regiones con lepra endémica. Los programas de trânsito libre entre los Estados Libres Asociados y los Estados Unidos, sin mediar mayores restricciones saltitarias, han creado nuevos problemas de salud pública. El grupo de casos de enfermedad de Hansen en Kona, Hawaii, USA, ilustra las dificultados para detectar y vigilar la diseminaeión do la enfermedad en las poblaciones inmigrantes. Este es un problema creciente que seguramente será más grave en los próximos anos. Se requieren métodos especiales y creativos para atacar el problema do la dotección, tratamiento y educación do casos on los grupos con diferencias culturales, de lenguaje y socioeconómicas. Los clínicos debcn permanecer alertas y preparados para el diagnóstico de la HD on los grupos do alto riesgo.Leprosy (Hansen's disease) is a significant health problem in many regions of the world. It affects over 1.2 million people throughout the world, with over 560,000 newly diagnosed cases every year (19). It remains endemic in 55 countries and is a major public health problem for countries in South and Southeast Asia, Africa and Latin America (16, 19).
Cases of Hansen's disease (HD) continue to be reported in the United States, with Hawaii, Texas, Louisiana, and California having the largest number of cases (12, 11, 15). Over 90% of the cases in the United States involve persons entering the country from endemic areas and are defined as imported (11, 15). Changing patterns of immigration, active refugee settlement, increased world travel and work abroad by American citizens have contributed to the changes in the number and distribution of HD cases in the United States. As of 1981,45 of the 50 states had reported at least one case of HD (15).
In 1986, the United States signed a Compact of Free Association with the former Trust Territories of the Republic of Marshall Islands and the Federated States of Micronesia. In late 1994, a Compact was also signed with the Republic of Palau. Together, these three states make up what is frequently called the Freely Associated States (FAS). The Compact directs relationships between the United States and the three island nations. Under the Compact, the United States funds the FAS for a range of development programs and authorizes the use of United States currency, federal processing of applications for air services, mail and other benefits, including immigration privileges.
Under immigration agreements, free travel between the United States and the FAS is allowed with no need for a visa, health screening or passport (2). There has been an increasing trend in the number of migrants from the FAS to the United States over the past few years. Whereas most of the Palauan migration has been to Guam and the Northern Mariana Islands, the major flow of the Marshall Islands' migration has been to Hawaii and the U.S. mainland (8). As of 1997, there were about 2500 Marshallese in Hawaii (7, 8).
In October 1996, a cluster of leprosy cases was found among a population of Marshallese immigrants in Kona on the island of Hawaii. We report on the demographics of this group and the results of subsequent contact investigations. We also discuss the impact of immigration on Hansen's disease in Hawaii and, in particular, the consequence of the new Compact of Free Association.
METHODS
The island of Hawaii, more commonly known as the Big Island, is the largest of the chain of islands comprising the state of Hawaii, U.S.A. With an area of 4200 square kilometers, it is dominated by three volcanic peaks. The Kona/Captain Cook area is located on the western coast with tourism and coffee as its two main industries.
In September 1996, a 19-year-old Marshallese male was admitted to Kona Hospital with complaints of nausea and vomiting. He was found to have sinusitis, giardiasis and lobar pneumonia. Tuberculosis was suspected but not confirmed. Because of skin findings, a skin biopsy was done. Active lepromatous leprosy (LL; according to Ridley-Jopling classification) was diagnosed on biopsy, and he was started on dapsone and rifampin. He was subsequently changed to the World Health Organization multibacillary (WHO/MB) treatment. In October, contact tracing was done. This screened an initial 28 household contacts for HD, and four more cases of HD were found among this group of 28. As a result of this, the screening program was expanded. Based on information that there was a larger population of Marshallese living in the same Kona/Captain Cook area, larger general screening clinics were set up. The general screening clinics included HD screening, tuberculosis screening, immunizations and hepatitis B evaluation.
By February 1997, three clinics had been organized in which a total of 237 individuals were screened. The clinics were staffed by the Hansen's Disease Community Program and the Big Island Public Health nurses and held over a period of 4 months.
RESULTS
Of the 237 Marshallese screened, a total of 11 cases of HD were identified by biopsy and started on treatment (The Table); 4 of the 11 had multibacillary (MB) disease. There were five males and six females with the oldest being 35 years old and the youngest 7 (mean age 17 years). Seven of the identified were of school-going age and attending public school in the Kona area. All of the 11 cases were from the Marshallese islands of Majuro or Enewetak and had arrived in the United States within the past 4 years.
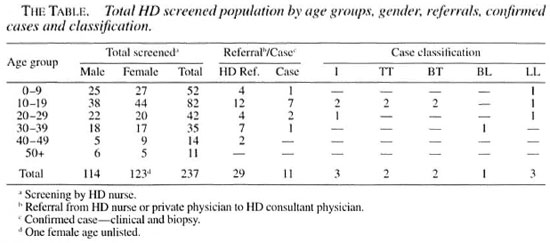
Of the 237 individuals screened, there were 114 males and 123 females; 75% were below the age of 30. The majority of the group came from the larger Marshallese islands of Enewetak and Majuro, with more than 60% arriving in Hawaii within the past 3 years. There was an increasing trend in the number of arrivals each year. Very few could speak English. The adults had minimal work skills for a developed country's economy and most were doing farm work. Living conditions were severely overcrowded with catchment systems for water supply and outhouses for sanitation needs. There was no telephone communication and transportation was poor and erratic. Approximately 40% had no medical insurance of any kind.
DISCUSSION
Compact of Free Association and current U.S. screening procedures for immigrants. Currently, both federal and state health regulations exist for the screening of immigrants to the United States for communicable diseases. At the federal level, the Immigration and Naturalization Service (INS) and the United States Public Health Service (USPHS) are the responsible agencies for ensuring that aliens arriving in the U.S. do not pose a threat to the public health of the country. The main instrument for accomplishing this is the visa medical examination. Prior to the issuance of an immigrant visa, every alien is required to submit to a medical examination. This is done by a physician in the country of origin, under contract with the INS/USPHS. The medical screening has as a general goal the exclusion of persons with communicable diseases of public health significance, persons with physical or mental health disorders associated with harmful behavior, persons who abuse drugs or are addicted to drugs, or persons who are likely to become a ward of the state. The current list of infectious diseases of public health significance that are grounds for exclusion include tuberculosis, human immunodeficiency virus (HIV) infection, Hansen's disease, and certain sexually transmitted diseases. Persons with diagnosed HD may be excluded from entry until they have received antimicrobial therapy for at least 6 months or are considered noninfectious (11, 13, 14). Even with this provision, the majority of imported HD cases are not detected at the time of entry (11).
In 1986, the Compact of Free Association was signed between the United States and the Marshall Islands. The Marshall Islands are a group of islands located in the North Pacific Ocean, about half way between Hawaii and The Philippines, with a population of about 61,000. Leprosy and tuberculosis and other health problems are endemic in the Marshall Islands. The prevalence rate of HD in the republic is 46.3 per 10,000 with a case detection rate of 2.1 per 100,000 population in 1997 (18). Multidrug therapy for the treatment of HD has been in use on the Islands since 1988 but, to the best of our knowledge, a leprosy elimination program has not yet been fully established in the country. Over-crowding, malnutrition and inadequate medical resources are other problems faced by the islanders.
As provided for in this treaty, travel between the Marshall Islands and the U.S. is free and unencumbered, with no need for a passport, visa or health screening. By allowing freedom of travel, the medical visa examination is waived, circumventing the primary tool for detecting communicable diseases.
In addition, the freedom of travel allowed under the agreement makes tracking of individuals from the FAS difficult. Being able to identify, quantify and locate target populations are key components in handling and preventing outbreaks or clusters of cases. There exist no accurate data on the number and location of Marshallese immigrants in the U.S. A census of Micronesian migrants to Hawaii in 1997 recorded about 2500 Marshallese in Hawaii (7, 8). According to data gleaned from Guam newspapers and from Marshallese community leaders and from the Marshall Islands Consulate in Hawaii, there were about 10,000 Marshallese migrants in the U.S. Most have migrated to Hawaii because of geographic reasons-proximity and better air links-and certainly for economic reasons. Large numbers have out-migrated to the Seattle, Washington area, Costa Mesa in California, and to areas in Oklahoma and Arkansas.
In addition, the number of Marshallese migrating to the United States has shown a consistently increasing trend in the years since the Compact was signed (7). Worsening economic conditions in the FAS have promoted greater migration. This trend is expected to continue if not accelerate before the anticipated renewal of the Compact in the year 2001.
A large number of the Marshallese migrants also routinely travel back and forth between the U.S. and the FAS each year. By doing so, they allow for the acquisition of new or reinfection, hampering communicable disease control and treatment (6). In a study of Asians in West Ham, U.K., 2% of immigrants infected with tuberculosis acquired infection during return visits to Asia (12). The size and the magnitude of this problem is difficult to assess because of the lack of travel data.
The ramification of the Compact of Free Association (CFA) may prove far-reaching. It impacts both public health and the economy of the state in which immigrants choose to settle. The main public health implications of the CFA are threefold: a) It has allowed for the circumvention of routine medical screening by incoming migrants; b) tracking and locating this group of migrants for the purpose of providing health care has been difficult, if not impossible, and c) temporary return migrants pose an additional source of possible new and re-infection.
Implications for Hawaii. Hawaii has a long history of imported cases of leprosy with the disease being introduced to the islands more than 150 years ago (21). It currently has a case detection rate of 1.8 new cases per 100,000, which is the highest in the United States (10). The vast majority represent imported cases of HD. The most recent example of this has occurred in Asians arriving following changes in U.S. immigration laws in 1965 which was followed by a large rise in imported leprosy cases, peaking in 1970-1980, then falling We could speculate that (as demonstrated by this cluster of cases) a new albeit more modest rise in imported HD cases may be expected with the continued arrival of migrants from the Freely Associated States and the Marshall Islands in particular (The Figure).
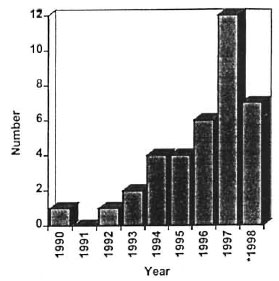
The Figure. Freely Associated States ID cases detected in Hawaii by year of detection. * = Figures for 1998 through June inclusive.
Although most (67.8%) imported HD cases in the United States are of the MB type and, therefore, potentially infectious, there is no evidence that imported cases result in transmission in the United States (11, 15). Despite the continued importation of HD into Hawaii, there has been no noted rise in secondary cases among the indigenous Hawaii-born population or among other ethnic groups (20). Similarly, in the United Kingdom, in spite of more than 1250 cases of HD imported since 1951, there have been no reports of consequent transmittal (4). This apparent lack of transmission may be due to a combination of factors, including improved nutritional status and better housing conditions resulting in decreased crowding in the United States. Malnutrition as well as prolonged and close contact with persons with MB disease are believed to be factors in the transmission of HD (5). The route of transmission is believed to be via nasal droplet infection in most cases (3, 9).
Early case finding is known to be the most important factor in preventing disability in leprosy (l7). Case detection of HD is often hampered by the immigrant's difficulty in accessing health care, due to language or cultural barriers or because of a lack of health insurance coverage. Stigmatization, belief in traditional medicine and the lack of formal education may also contribute to delays in presentation and treatment (1).
With the bypass of medical screening procedures and the lack of information on the number and location of FAS migrants in Hawaii, efforts in providing health screening to this group present a unique problem unto itself. Directed searches to find and offer medical care and education may be construed as discriminatory. Overt public screening efforts could lead to stigmatization and social marginalization that would prove counterproductive.
A community-based approach has been advocated and implemented in Hawaii. Health and social welfare workers acting through selected church groups have been able to locate and reach out to the FAS migrants. Voluntary health screening is offered along with education regarding immunization, HD, tuberculosis and hepatitis. Through this novel approach, larger communities of Marshallese and other Micronesians have been located and screened. These efforts are currently ongoing. Educational efforts through the distribution of pamphlets with information on health services have also been initiated for incoming FAS visitors at the international airport, the main port of entry for FAS migrants. These pamphlets offer information on disease and health care services for voluntary health screening and treatment.
Targeting a single disease such as HD ignores other significant health problems or leads to the discovery of problems for which public resources may not be available. In this cluster of cases, case detection and screening work were conducted principally by the State of Hawaii Hansen's Disease Branch. Besides HD, a significant percentage of the Marshallese screened were found to have other concurrent diseases, such as hepatitis. These diseases fell outside the scope of the HD Branch and providing treatment for them proved to be an added dilemma. Because 40% of those screened lacked medical insurance, financial and medical assistance was wanting. Only through extraordinary measures were public funds and resources mustered. Future screening efforts of immigrant populations in the U.S. must, therefore, make provisions for the treatment of a wide range of possible diseases; this is especially so in groups known to come from areas in which these diseases are endemic.
Lastly, the role of community-based physicians in any HD surveillance program cannot be overemphasized. This cluster of cases was discovered rather fortuitously through the effort of an alert community- based practitioner. Because of the disease's long incubation period and myriad presentations, physicians must be vigilant and keep the diagnosis of leprosy in mind for many years after immigrants have entered into the United States, especially if they are from endemic areas.
REFERENCES
1. Bekri, W., Gkbre, S., Mengiste, A., Saunderson, P. R. and Zewge, S. Delay in presentation and start of treatment in leprosy patients: a case-control study of disabled and non-disabled patients in three different settings in Ethiopia. Int. J. Lepr. 66(1998)1-9.
2. Compact oi Free Association Act of 1995 (FSM). Public Law 99-239. January 14. 1996. 99th U.S. Congress. Title 1 Act 4 Section 141.
3. Davey, T. F. and Rees, R. J. W. The nasal discharge in leprosy: clinical and bacteriological aspects. Lepr. Rev. 45(1974)121-134.
4. Dockrell, II. M, Eastcott, H., Young, S., Mac- Farlane, A., Hussain, R. and Waters, M. F. R. Possible transmission oi Mycobacterium leprae in a group of U.K. leprosy contacts. Lancet 338(1991)739-743.
5. Fine, P. E. M. Leprosy-the epidemiology of a slow bacterium. Epidemiol. Rev. 4(1982)161-188.
6. Gellert, G. A. International migration and control of communicable diseases. Soc. Sci. Med. 37(1993)1489-1499.
7. Impact of The Compact of Free Association on thf: United States. Washington, D.C.: Office of Insular Affairs, U.S. Department of the Interior, January 1998.
8. Levin, M. J. Micronesian Migrants to Hawaii, Guam and the Commonwealth of the Northern Mariana Islands; A Study of the Impact of the Compact of Free Association . Appendix A. Washington, D.C.: International Programs Center, Population Division, U.S. Bureau of the Census, 1998.
9. Mandell, G. L., Bennet, J. E. and Dolin, R.. eds. Mandell, Douglas and the Bennett Principles and Practice of Infectious Diseases . 4th edn. New York: Churchill Livingstone, 1995, 2243-2250.
10. Maruyama, M. Hansen's disease in Hawaii. State of Hawaii Department of Health Commun. Dis. Rep. January/February (1994)1-3.
11. Mastro, T. D., Redd, S. C. and Breiman, R. F. Imported leprosy in the United States, 1978 through 1981: an epidemic without secondary transmission. Am. J. Public Health 82(1992)1127-1130.
12. McCarthy, O. R. Asian immigrant tuberculosis; the effect of visiting Asia. Br. J. Dis. Chest 78(1984)248-253.
13. Medical examination of aliens. Federal Register 56(1991)2484.
14. Medical examination of aliens. Federal Register 56(1991)2500.
15. Neill., M. A., Hightower, A. W. L. and Broome, C. V. Leprosy in the United States, 1971-1981. J. Infect. Dis. 152(1985)1064-1069.
16. Noordeen, S. K. Leprosy control through multidrug therapy-update. Bull. WHO 69(1991)263-269.
17. Richakdus, J. H., Finlay, K. M., Croft, R. P. and Smith, W. C. S. Nerve function impairment in leprosy at diagnosis and at completion of MDT: a retrospective cohort study of 786 patients in Bangladesh. Lepr. Rev. 67(1996) 297-305.
18. WHO Action Programme for the Elimination of Leprosy. Status report update 1997. Geneva: World Health Organization, 1997.
19. WHO Action Programme: for the Elimination of Leprosy. Program Managers Meeting, Guam, August 1997. Geneva: World Health Organization. 1997.
20. Worth, R. M. Leprosy in Hawaii; the end of an epidemic. (Editorial) Int. J. Lepr. 64(1996)441-447.
21. Worth, R. M. and Bomgaars, M. R. Immigration and leprosy in Hawaii, 1960-1981. Int. J. Lepr. 50(1982)335-341.
1. M.D.; Department of Medicine, University of Hawaii, 1356 Lusitana Street, 7th Floor, Honolulu, Hawaii 96813-2427, U.S.A.
2. M.D., M.P.H.; Department of Medicine, University of Hawaii, 1356 Lusitana Street, 7th Floor, Honolulu, Hawaii 96813-2427, U.S.A.
3. M.P.H., Department of Medicine, University of Hawaii, 1356 Lusitana Street, 7th Floor, Honolulu, Hawaii 96813-2427, U.S.A.
Reprint requests to Dr. Frankel at the above address or FAX 1-808-586-7486.
Received for publication on 31 August 1998.
Accepted for publication in revised form on 15 December 1998.