- Volume 67 , Number 2
- Page: 129–32
Reanimation of the lagophthalmos using stainless steel weight implantation; a new approach and prospective evaluation
ABSTRACT
Weight implants have been used for over 30 years in surgical rehabilitation following lagophthalmos. However, there has been a renewed interest among ophthalmologists in recent years. The weight implant technique combined with lateral canthus resuspension was performed on 22 eyes in Thai patients. It is a reliable method for correcting lagophthalmos and ectropion. In previous studies almost pure gold was used in 99.99% of eyelid implants. However, we wanted to use other materials which are not expensive and are readily available. A stainless steel plate was selected. The majority of our surgeries were done with a stainless steel weight implant of 1.368 g. Patients were followed for 7 to 55 months, and no rejections of the implants were observed. This study achieved a >90% success rate, and showed that a stainless steel plate is an alternative to gold for the weight implant technique.RÉSUMÉ
Depuis plus de 30 ans, une technique chirurgicale, qui utilise de prothèses augmentant le poids des paupières, restaure les fonctions palpébrales altérées lors de lagophtalmies. Cette procédure a bénéficié ces dernières années d'un regain d'intérêt parmi les ophtalmologistes. Cette technique d'implant, combinée à une resuspensiôn de l'angle latéral delà paupière, fut pratiquée sur 22 yeux de patients thaïlandais. Cette méthode est sûre et efficace pour corriger les lagophtalmies et les ectropions. Dans les travaux précédants, 99.99% des implants palpébraux était constitué d'or quasi-pure. Cependant, nous avons voulu utiliser d'autres matériaux moins chers et plus faciles à obtenir. Une plaque en acier inoxydable fut retenue. La majorité des chirurgies ont été faites avec des prothèses en acier inoxydable pesant 1.368 grammes. Les patients furent suivis pendant une période de 7 à 55 mois, et aucun rejet d'implant ne fut observé. Cette étude eut un taux de succès de plus de 90% et démontre qu'une plaque en acier inoxydable est une alternative à une plaque en or dans la technique chirurgicale utilisant des prothèses dont la fonction est d'augmenter le poids des paupières.RESUMEN
Aunque los implantes de peso se han usado por más de 30 anos en Ia rehabilitación quirurgica del pár- pado de pacientes con lagoftalmos, en los últimos anos ha habido un renovado interés entre los oftalmólogos por esta técnica. La técnica dei implante de peso, combinada con Ia resuspensión dei cantus, fue practicada en 22 ojos de pacientes Thai. Esta técnica es un pro- cedimiento confiable para corregir el lagoftalmos y el ectropion. Aunque en el 99.99% de los estúdios prévios se ha utilizado el oro puro para fabricar los implantes de peso, nosotros quisimos usar otros materi- ales que fueran más baratos y de fácil adquisición. Se seleccionó así el acero inoxidable en placas de 1.368 g. Los pacientes se supervisaron durante 7 a 55 meses y no se observaron rechazos de los implantes. Este estúdio alcanzó un grado de êxito mayor al 90% y demostro que la plaça de acero inoxidable es un buen substituto del oro en los implantes de peso.Estimating the number of leprosy patients affected with lagophthalmos is problematic. It has been shown that, at a minimum, 2% of paucibacillary patients (2) and 5% of multibacillary patients have lagophthalmos. Lagophthalmos is a serious complication of leprosy and a significant cause of ocular morbidity in leprosy. Surgical intervention is the only method for correcting lagophthalmos and preventing corneal disease and vision loss.
There are a number of different surgical procedures for the correction of lagophthalmos (1). Results from a survey of eye care revealed that the surgery most commonly used for correction of lagophthalmos was tarsorrhaphy. Surgeons in Africa relied almost exclusively on this procedure, while surgeons in Asia reported using tarsorrhaphy, horizontal shortening and temporalis muscle transfer (TMT) almost equally. Many of the surgical techniques previously described, unfortunately, have unwanted cosmetic drawbacks. They may produce unsightly local facial scars and obstruct peripheral vision, and they may not provide adequate corneal protection.
Techniques for rehabilitating lagophthalmos include both static and dynamic procedures (4). Static procedures include fascial or alloplastic slings, brow lift, canthoplasty and lid tightening. Dynamic procedures include regional muscle transposition, that is, temporalis, masseter, and various eyelid reanimating procedures, such as gold-weight lid loading, eyelid spring implantation and Silastic™ encircling prosthesis implantation, all of which focus on the restoration of eyelid closure. If the TMT procedure is done by an experienced surgeon, the result is good. But the procedure requires an extensive learning period before an optimal result can be reached. Unwanted results, for example, ectropion, entropion, over-tightening and laxity, over the long run are of major concern, and repeat surgery is difficult.
This paper suggests another technique that is not as complex as TMT but has a good result. This surgical technique which includes eyelid reanimation with a prosthetic device by loading the upper eyelid to provide gravity-assisted closure in cases of lagophthalmos was initially described by Illig in 1958 (3). He stated that "the principle is the replacement of the lost tonus of the orbicularis oculi muscle by a small gold weight which, covered by a nonirritating material, is implanted into the upper eyelid." The procedure is based on the fact that the upper eyelid provides significantly more of the actual closure in coverage of the cornea than the lower eyelid.
In 1966, Smelli (5) reported the use of a lead-based lid load to replace the orbicularis function. He thought that a number of metals, including gold, lead, stainless steel, tantalum and platinum, would be satisfactory for the implants because of their high density, availability, and malleability. He also concluded that the "lid loading operation has the merit of simplicity and probably a unique advantage in that the surgeon is able to assess the result before the operation is performed merely by attaching the weight to the skin of the upper eyelid." He thought that this procedure had an important advantage over the temporalis muscle transplant, a procedure popular at that time, since lid loading did not interfere with the normal blinking reflex.
May (4) reported a total of 94 patients treated with the lid-loading technique with a 2-year follow up. The success rate was 91%; the 9% failure rate was related to residual lagophthalmos or unacceptable ptosis. In addition, Townsend (7) presented the results of gold-weight eyelid implantation over a 15-month period in 23 patients. A 92% success rate was obtained (average follow up 12 months).
At present, pure 24-K gold and tantalum are used as the eyelid weights, but very little is known about stainless steel. A stainless steel implant was used in this study because it is not expensive and is readily available.
MATERIALS AND METHODS
A total of 20 Thai patients undergoing reanimation surgery for lagophthalmos in Phra-Pradaeng Hospital in Thailand, between January 1993 and February 1998, were studied prospectively. Of the 20 patients there were 18 leprosy patients and two patients without leprosy (four females and 16 males). Only one eye was operated on in each of 18 patients and both eyes in two patients were operated on for a total of 22 eyes. The patients ranged in age from 29 to 65.
Indications for surgical intervention included ocular findings of significant lagophthalmos with exposure keratopathy being present despite standard medical therapy, patients noncompliant with medical therapy, and monovision on the paralytic side.
An ocular evaluation of each patient included: visual acuity, degree of exposure keratitis, lagophthalmos, presence of Bell's phenomenon, eyelid palpebral fissure distances, levator function and checking for the absence of exophthalmos.
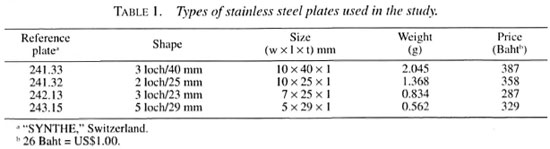
In previous studies, a gold plate had been used to correct lagophthalmos (weights ranging from 0.6 to 2.6 g at 0.2 g intervals). Further trials found that a stainless steel plate needed to have the following three properties: a) weight range between 0.6 g and 2.6 g; b) a rectangular shape; c) size no larger than the upper eyelid. While an orthopedic plate with the above properties is a solution, it is not commercially available in the proper serial weights. Table 1 shows four types of plates that were selected for this study. Before surgery, two orthopedic bending irons were used to compress the stainless steel plate, bend it to conform to the upper eyelid contour, and to test the proper weight in each patient.
Surgical procedure. Each patient was tested pre-operatively by taping the weight implant to the affected upper eyelid(s) to determine the weight necessary to provide adequate closure of the lid, with a ptosis of not more than 1.5 mm. Surgery was performed under local anesthesia using 2% lidocaine with epinephrine infiltrated into the upper eyelid along the lid crease and at the lid margin edge. A 15 Bard-Parker blade was used to incise the skin and Westcott scissors were used to enter the orbicular plane, which was elevated from the underlying orbital septal plane and tarsal plate. A stainless steel plate was inserted into the pocket between the orbicularis muscle and the orbital septum-tarsal plate. The lower part of the pocket was sutured to the superior tarsal border and the upper part was sutured to the orbital septum, using a 6-0 silk suture passed through the pre-formed holes in the plate. The length of the plate varied with the weight of the implant. The plate was set over the medial two thirds of the superior tarsal border; if more plate length was needed the lateral part was extended. The overlying orbicular muscle was sutured together using a 6-0 absorbable suture, and the skin was then closed with interrupted 6-0 silk sutures. Post-operative sleep was in a supine position with the head tilted up 30°. In patients with lower eyelid ectropion, lateral canthal resuspension (tightening) was done. This was performed frequently in this series, and some patients went on to treatment with a subsequent stage of lateral canthal tightening.
RESULTS
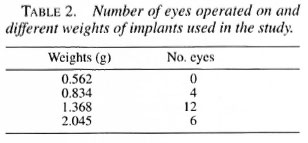
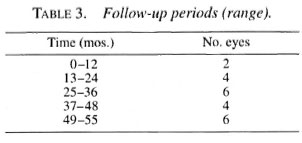
In the study the weight most commonly used was 1.368 g (Table 2). The follow-up period and time range was 7 to 55 months (Table 3). After more than 12 months of follow up, 20 of the 22 eyes were still in good condition. In two eyes after 7-8 months, the plates were removed due to thinning of the skin and tightening of the lid.
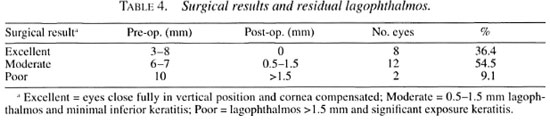
Post-operative results are shown in Table 4. The surgery was graded as excellent if complete closure was obtained, moderate if a residual eyelid palpebral fissure distance of 0.5-1.5 mm persisted. Both excellent and moderate results are accepted as a success, and the success rate is, therefore, about 90% in this study, which is about the same as the success rates in previous studies. Poor results were found in one patient who lacked sufficient upper eyelid skin and the plate extruded, and in another patient who had tight upper eyelid skin or eyelid scarring.
DISCUSSION
This study has shown that satisfactory surgical results can be obtained with the use of the weight implant technique. A success rate of >90% has been achieved. A poor result in one case was due to skin thinning and plate extrusion. This patient was reop- erated to remove the plate, and a non-epithe- lialized capsule of fibrous tissue was found around the plate. This tissue had filled the hole along the contour of the plate. In cases with excellent results, some of the patients with previously keratinized corneas were noted to have the keratinization disappear.
The advantage of this surgical technique is that it is a relatively straightforward technique that is familiar to ophthalmic surgeons. Readjustment of the prosthesis usually is not necessary once the weight and technique are optimal. This procedure does not require physical therapy for success, and has a good cosmetic effect, i.e., an oval- not round-shaped lid fissure. On the average, the final result can be assessed pre- operatively. Post-operative complications, such as ectropion (6), entropion and overtightening, were not found in this study. Finally, if there are some post-operative problems, removal of the plate is simple, and the weight can be increased or decreased easily on follow-up surgery.
The disadvantages include the possibility of infection and extrusion. However, this has represented a potential rather than a real problem in both this study and other studies to date. There is also some concern about cosmetic appearance. If the weight implant is placed too superficially, it may resemble a chalazion-like subcutaneous lump in the eyelid. The patient may have an ongoing need for topical lubricant drops and ointments. Some patients have developed increased and variable astigmatic refractive error related to the gravitational effect of the weight implant over the corneal surface curvature.
There were no signs of inflammation in any of the 22 eyes during the period of follow up. Pure gold (medical grade) is expensive, and there is a problem in availability, but it is the best material if the patient can afford it. Stainless steel is the alternative choice because it is inexpensive, readily available, and produces a favorable result.
Acknowledgment. I thank Dr. Suchat Kulkosa, Previous Head, Ophthalmology Section, Phra- Pradaeng Hospital, who kindly allowed publication of the outcome of this study for his valuable comments. Also, I thank Dr. Kowit Kampirapap, who critically read and revised the manuscript.
REFERENCES
1. Courtright, P. and Lewallen, S. Current concepts in the surgical management of lagophthalmos in leprosy. Lepr. Rev. 66(1995)220-223.
2. Hogeweg, M., Kisan, K. U. and Suneetha, S. The significance of facial patches and type 1 reaction for the development of facial nerve damage in leprosy; a retrospective study among 1226 paucibacillary leprosy patients. Lepr. Rev. 62(1991)143-149.
3. Illig, K. M. Eine neue operationsmethode gegen lagophthalmos. Klin. Monalsbl. Augenheilkd. 132(1958)410-411.
4. May, M. Gold weight and wire spring implants as alternatives to tarsorrhaphy. Arch. Otolaryngol. Head Neck Surg. 113(1987)656-660.
5. Smelli, G. D. Restoration of the blinking reflex in facial palsy by a simple lid load operation. Br. J. Plast. Surg. 19(1966)279-284.
6. Soares, D. and Chew, M. Temporalis muscle transfer in the correction of lagophthalmos due to leprosy. Lepr. Rev. 68(1997)38-42.
7. Townsend, P. J. Eyelid reanimation for the treatment of paralytic lagophthalmos. Ophthal. Plast. Reconstr. Surg. 8(1992)196-201.
M.D., Ophthalmology Section,Phra-Pradaeng Hospital, Poochaosamingprai Road, Phra-Pradacng, Samuthprakarn 10130, Thailand.
Received for publication on 17 November 1998.
Accepted for publication in revised form on 1 March 1999.
The author has no proprictary interest in the materiais or products presented.