- Volume 68 , Number 1
- Page: 23–6
Pathology of a lepromatous eye
ABSTRACT
Histopathological examination of an enucleated eye f rom a lepromatous leprosy patient showed the cornea, ciliary body, and part of the choroid to be infiltrated by macrophages filled with Mycobacterium leprae. The walls of blood vessels in the sclera, ciliary body and the anterior choroid demonstrated the presence of M. leprae, giving credence to the blood-borne entry of M. leprae into the eye. Unlike the eyes of experimental animals infected with M. leprae, histopathological study of this eye f rom a lepromatous leprosy patient demonstrated that M. leprae, although demonstrable in the anterior choroid, could not be found in the posterior parts of the eye, substantiating the claim that leprosy docs not affect the posterior parts of the eye directly.RÉSUMÉ
L'examen histopathologique à la suite de l'énucléation d'un oeil d'un patient souffrant de lèpre lépromateuse, a montré des infiltrats de macrophages emplis de Mycobaclerium leprae dans la cornée, les corps ciliaires et dans une partie de la choroïde. Les parois des vaisseaux sanguins de la sclère, les corps ciliaires et la partie antérieure de la choroïde contenaient des M. leprae, supportant l'hypothèse de l'entrée de M. leprae dans l'oeil par voie sanguine. A la différence des yeux étudiés dans les modèles expérimentaux d'infection par M. leprae, l'examen histopathologique de cet oeil provenant d'un patient souffrant de lèpre lépromateuse a montré que M. leprae, quoique présentes dans la choroïde antérieure, ne pouvaient pas être trouvées dans les parties plus postérieures de l'oeil, supportant la possibilité que la lèpre n'affecte pas le segment postérieur de l'oeil directement.RESUMEN
El examen histopatológico de un ojo enucleado de un paciente con lepra lepromatosa mostró que la córnea, el cuerpo ciliar y parte del coroides estuvieron infiltrados por macrófagos repletos de Mycobacterium leprae. Las paredes de los vasos sanguíneos en la esclera, el cuerpo ciliar y el coroides anterior mostraron la presencia de M. leprae, sustentando la idea de que la infecciôn del ojo ocurre a través de la sangre. A diferenci a de los ojos de animales infectados experimentalmente con M. leprae. el estudio histopatolôgico del ojo de este paeiente lepromatoso mostrô que antique M. leprae puede estar présente en el coroides anterior, generalmene no se encuentra en las partes posteriores del ojo, apoyando el reelamo de que la lepra no alecta directamente las partes posteriores del ojo.It is estimated that between a quarter and a hall million leprosy patients have Grade 2 visual disability. One fifth of all leprosy patients have potentially sight-threatening lesions (4). Publications on ocular leprosy are not proportionate with the high prevalence of ocular complications and are mainly based on clinical observations. Reports of histopathologicy studies on lepromatous lesions of the eye are few. Histopathological investigations done on intact and entire eyeballs which have been removed from leprosy patients cither during enucleation or at autopsy (2) are scarce. This may be because whole eyeballs are difficult to obtain. On the other hand, there have been many studies done on ocular tissues of armadillos experimentally infected with Mycobacterium leprae (1, 5- 7). We examined the enucleated, entire eyeball of a lepromatous patient histopathologically and report our findings in this paper.
CASE REPORT
A 40-year-old, lepromatous leprosy patient who had bilateral lagophthalmos and repeated iridocyclitis in both eyes and who had been treated with dapsone monotherapy for 25 years presented with a painful right eye which was not responding to medical therapy. The right eye had a complete corneal opacity with a small, firm, round, white nodule about 3 mm in diameter attached to the six o'clock limbus. Details of the inner tissues of the eye could not be made out because of the corneal opacity. This eye, which had no perception of light, was enucleated after repeated requests from the patient and after written consent was obtained. At the time of enucleation the patient had an average bacterial index (BI) of 2.40+ with 5.00-f in the buttock and ear. The enucleated right eye was sent for histopathological examination.
HISTOPATHOLOGY
The intact ocular globe was first fixed in 10% formalin for 24 hr and then cut open along the horizontal plane from back to front. Serial sections 5-µm thick were made; some were stained with hematoxylin and eosin (H&E), others with a modified Fite-Faraco stain for acid-fast bacilli (AFB).
Histopathological examination showed that the upper half of the corneal stroma had focal degeneration and calcification. The lower half of the corneal stroma showed large inflammatory cell collections consisting of foamy macrophages, lymphocytes and plasma cells (Fig. 1). Diffuse collections of iris (melanin) pigment were also seen on the lower half of the corneal stroma, and parts of the iris were seen to be adhering to the back of the cornea. Few M. leprae were seen in the epithelial layer, but the stroma contained numerous clumps of M. leprae within macrophages (Fig. 2). At the limbus, focal collections of macrophages were seen around blood vessels. The episcleral and scleral blood vessels were found to be dilated and congested. A few macrophages surrounding the dilated blood vessels were seen only in the sclera covering the anterior portion of the eye. There was dense infiltration by macrophages, lymphocytes and plasma cells in both the iris and ciliary body (Fig. 3). There was complete distortion of the architecture at the level of the angle of the anterior chamber and the trabecular meshwork. There was almost complete destruction of the ciliary muscles. Foamy macrophages were seen on the anterior portion of the lamina fusca layer of the choroid, some of them containing M. leprae. Some of the choriocapillarics showed bacilli (Fig. 4). A clump of AFB was also seen in a nerve twig in the choroid (Fig. 5). The choroid beyond the equator of the eye was devoid of macrophages or M. leprae. The lens, vitreous, retina, optic nerve and external eye muscles did not show any significant pathology.
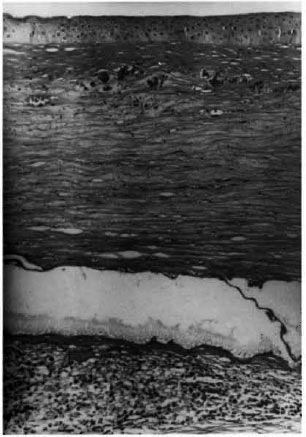
Fig. 1. Photomicrograph of the corneal epithelium and stroma showing focal calcium precipitation. Sheets of foamy macrophages are seen in the posterior stroma (H&Ex 100).
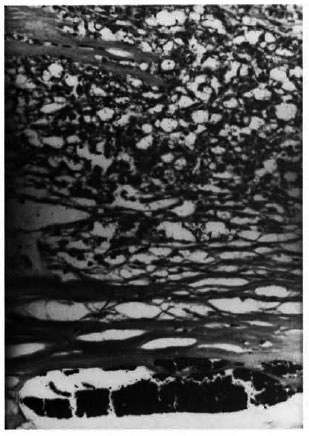
Fig. 2. Photomierograph showing corneal stromawith iris pigments. Colleetions of foamy macrophageswith elumps of M. leprae are also seen (acid-fast stainx200).
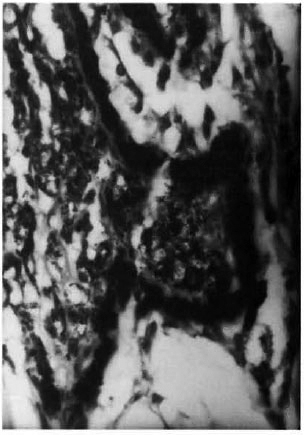
Fig. 3. Photomicrograph showing a ciliary processwith clusters of macrophages containing M. leprae (aeid-fast stain x400).
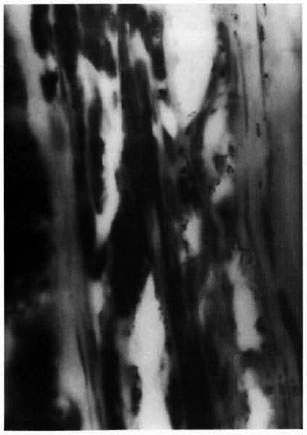
Fig. 4. Photomicrograph showing the choriocapil-lary layer. Scattered M. leprae are seco ou the wall ofblood vessels ( acid-fast stain x1000).
Fig. 5. Photomicrograph showing a clump of AFBin a nerve twig in the choroid (acid-fast stain x1000).
DISCUSSION
Although clinically it is recognized that the posterior portion of the eye is not affected by leprosy, there have been a few histopathological reports that have described the presence of AFB in the retina (3,8). The histopathological study done on the eye of this smear-positive, lepromatous patient with active disease substantiates two primary beliefs in ocular leprosy. The spread of leprosy to the eye is thought to be blood borne. This is supported by the fact that the walls of blood vessels of the limbus, ciliary body, iris and the choriocapillarics demonstrated the presence of M. leprae. The posterior part of the eye is purported to be warmer by about 6ºC than the anterior part of the eye (9), and cooler temperatures have been linked with the growth and pathogenicity of M. leprae. In this smear-positive, lepromatous patient the cornea, iris and ciliary body were loaded with AFB. The sclera and the choroid of the anterior portion of the eye showed numerous AFB, but a diligent and laborious search in several sections of the eye failed to demonstrate any AFB in the sclera or choroid beyond the equator of the eyeball. The gradual disappearance of macrophages and AFB as the ocular tissues extend posteriorly and the total absence of AFB in the retina, vitreous and the optic nerve corroborates the temperature linkage of the growth of M. leprae in the ocular tissues. It is also a representation of the significant difference seen between humans and armadillos infected with M. leprae. The choroid and retina of the armadillos were found to be heavily infiltrated with M. leprae, even in the posterior parts of the eye (1).
REFERENCES
1. BRANDT, F., ZHOU, H. M., SHI, Z. R., KADZDA, J., DHOPLIE, A. M., KOLK, A. and SCHMIDT, D. S. The pathology of the eye in armadillos experimentally infected with Mycobacterium leprae. Lepr. Rev. 61 (1990) 112-131.
2. DESIKAN, K. V. and JOB, C. K. Report on the study of eye lesions in three autopsied cases of leprosy. Lepr. India 42 (1970) 2-3.
3. ELLIOT, D. C. Further report on the polypoid leprous lesions of fundus, 6 cases. Int. J. Lepr. 17 (1949) 229-236.
4. FEYTCHE, T. J. The prevalence of disabling ocular complications of leprosy: a global study. Indian J. Lepr. 70 (1999) 49-59.
5. MAI.ATY, R. and Tongni, B. Corneal changes with nine-banded armadillos with leprosy. Invest. Ophthalmol. Vis. Soc. 29 (1988) 140-145.
6. MALATY, R., Walsh, G. P., Mkylks, W. M., BiniOKI), C. H. and Jon, C. K. Ocular leprosy in ninebanded armadillos. Invest. Ophthalmol. Vis. Sei. 27 (1986)38.
7. McDOUGALL, A. C. and REES, R. J. W. Ocular histopathology in animals experimentally infected with Mycobacterium leprae and M. lepraemurium. 2. Mycobacterium leprae infections in the 9-banded armadillo (Dasvpus itovemcinctus L.). Br. J. Ophthalmol. 62 (1978) 516-524.
8. OREFICE, F., Miranda, D. and Boratto, L. M. Presence of M. leprae in the conjunctiva, vitreous body and retina of a patient having lepromatous leprosy. Indian J. Lepr. 70 (1998) 97-102.
9. SCHWARTZ, B. Environmental temperature and ocular temperature gradient. Arch. Ophthalmol. 74 (1965) 237-243.
1. M.D., Head, Department of Histopathology and Experimental Pathology.
2. M.S., D.O., Head, Department of Ophthalmology, Schieffelin Leprosy Research and Training Center, Karigiri, Vellore District, Tamil Nadu, India 631106.
Received for publication on 23 September 1999.
Accepted for publication on 14 December 1999.