- Volume 68 , Number 2
- Page: 182–4
Disabilities in leprosy
To the Editor:
Even with successful treatment, the leprosy patient is frequently left with various disabilities and deformities which result in social boycott of the patient.
Disabilities and deformities frequently remain a grim remainder of the disease even after successful treatment. Disability rates reported from various centers vary greatly because of the type of leprosy prevalent and the criteria followed for labeling disabilities. The second report of the World Health Organization (WHO) Expert Committee on Leprosy estimated that about 25% of leprosy patients have some degree of disabilities (8). In our retrospective study (1971-1993) after going through the records of an urban leprosy clinic, we evaluated the disabilities of 180 patients.
The disabilities for hands, feet, eyes and face were recorded for 180 patients who attended the urban leprosy clinic during the study period and who were classified on the Ridley-Jopling scale. A disability index-2 (DI-2) was calculated for the hand, foot and eye only using the method suggested by Bechilli and Martinez-Dominguez (1). A score of 1 was given for grade I disability, 2 for grade II and 3 for grade III disability. All three disability scores were added and divided by 6 to get the DI-2. The data for this disability study were analyzed using simplified classification of leprosy, i.e., lepromatous, borderline and nonlepromatous leprosy.
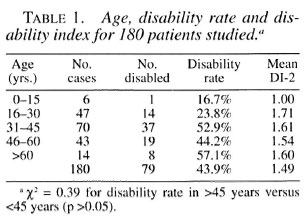
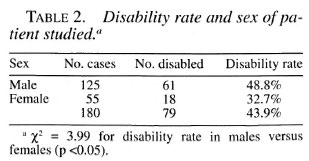
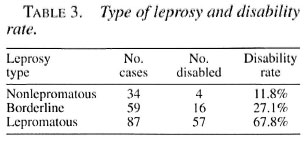
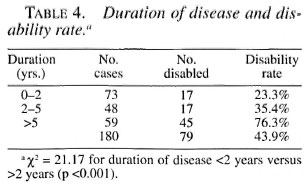
The disability rate was found to be the highest in the age group above 60 years (57.1%), followed by 52.9% in the group 31-45 years. The disability rate was lowest in those 0-15 years (16.7%) (Table 1). Table 2 shows the disability rate and sex of the patients. The disability rate was higher in males (48.8%) than in females (32.7%). As shown in Table 3, the disability rate was highest in lepromatous leprosy (67.8%) and lowest in nonlepromatous leprosy (11.8%). The duration of disease and the disability rate were directly proportional to each other; as the duration of leprosy advanced the disability rate also increased (Table 4).
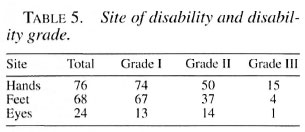
Hands were the most common site of disability in all disability grades, followed by the feet and eyes. The larynx was involved in 3% of the cases, collapse of the nose was seen in 15% and facial palsy in 5% (Table 5).
Rao, et al. (3) in Karigiri, South India, found the disability rate to be 42.9%. Kushwah, et al. (2) in Gwalior, India, found the disability rate to be 30.2%. Reddy and Bansal (4) in Pondicherry, India, observed the disability rate to be 16% and Sehgal and Sharma (6) in Delhi found the disability rate to be 30%. Saha and Das (5) found the disability rate to be 22% in Calcutta. The highest disability rate and index in our study are mainly due to the large number of lepromatous and borderline leprosy cases - 87 (48%) and 59 (32%), respectively.
The disability rate in our study was significantly higher (p <0.05) in males (48.8%) as compared to females (32.7%). Also, it was higher in older patients than in younger ones. Similar observations were also noted by the other studies compared above. The disability index was significantly higher (p <0.001) in those with a duration of disease more than 2 years (58%) as compared to those with a disease duration of less than 2 years (23%). These findings are consistent with those of Sehgal and Sharma (6), Thappa, et al. (7) and Saha and Das (5). Males, by virtue of their occupations, outdoor habits and smoking, are more likely to be injured.
The disability rate in our study was highest in lepromatous cases (67.8%), least in nonlepromatous cases (11.8%) and intermediate in borderline cases (27.1%). These findings are consistent with those of Reddy and Bansal (4), and Saha and Das (5). The hands and feet were involved most frequently in our study. Anesthesia of extremities, i.e., grade I, was the commonest disability seen. This is parallel to the studies by Thappa, et al. (7) and Saha and Das (5).
- G. Kalla, M.D., M.N.A.M.S.
Dilip Kachhawa, M.D.
Atul Salodkar, M.D.
Department of Dermatology, STD and Leprosy
Dr. S.N. Medical College
Jodhpur (Raj.), India
REFERENCES
1. Bechelli, L. M. and Martinez-Dominguez, V. Disability index for leprosy patients. WHO Bull. 44 (1977)709-713.
2. Kushwah, S. S., Govila, A. K. and Kushwam, J. An epidemiological study of disabilities among leprosy patients attending leprosy clinic in Gwalier. Lepr. India 53 (1981) 240-246.
3. Rao, P. S. S., Karat, A. B. A., Karat, S. and Furness, M. A. Prevalence of deformities and disabilities among leprosy patients in an endemic area. Part-1 General findings. Int. J. Lepr. 38 (1970) l-11.
4. Reddy, B. N. and Bansal, R. D. An epidemiological study of leprosy disability in a leprosy endemic rural population of Pondicherry (South India). Indian J. Lepr. 56(1984) 191-194.
5. Saha, S. P. and Das, K. K. Disability pattern amongst leprosy cases in an urban area (Calcutta). Indian J. Lepr. 65 (1993) 305-314.
6. Sehgal, V. N. and Sharma, P. K. Patterns of deformities/disabilities in urban leprosy. Indian J. Lepr. 57(1985) 183-197.
7. Thappa, D. M.. Kaur, S. and Sharma, V. K. Disability index of hands and feet in patients attending an urban leprosy clinic. Indian J. Lepr. 62 (1990) 328-337.
8. WHO Expert Committee on Leprosy. Second report. Geneva: World Health Organization, 1960. Tech. Rep. Ser. 459.
Reprint requests to Dr. G. Kalla, 4-F-12 New Power House Road, Jodhpur 342003, India.