- Volume 68 , Number 2
- Page: 186–92
News and notes
This department furnishes information concerning institutions, organizations, and individuals en gaged in work on leprosy and other mycobacterial diseases, and makes note of scientific meetings and other matters of interest.
Ethiopia. ALERT Tuberculosis Program Managers Course. Information on a Tuberculosis Program Managers Course offered by ALERT 16 October-3 November 2000 is given below.
Target audience: Health managers responsible for tuberculosis (TB) control activities at the national or intermediate level in governmental or nongovernmental organizations.
Lecturers: Lecturers and facilitators will be TB-Public Health Specialists from ALERT and the Nuffield Institute for Health (NIH) with national and international experience in the planning and management of TB control programs.
Venue: Course will be held at the ALERT Training Center, Addis Ababa, Ethiopia.
Course development: The core course has been developed based on a training needs assessment and task analysis by the Epidemiology Unit of the Catholic University of Louvain (UCL) in Belgium with funding from the Damien Foundation and by the NIH in the U.K. with funding from the U.K. Department for International Development (DFID).
Course design: The 15-day course uses a problem-oriented learning method, includes actual case studies as the basis for practical exercises, and seeks to build on the experience and input of participants.
Course structure and content: The course modules are organized around the stages of the program management cycle. A variety of issues related to situation analysis, strategy development and option appraisal, planning and implementation, supervision, monitoring and evaluation will be addressed.
Course fees: Full course fee (excluding air fares and visa costs) is US$2,080.
Applications: Please note that enquiries and applications need to be made as soon as possible. Application forms must be submitted no later than 20 August and participants will be notified of acceptance no later than 10 September. Application forms may be requested and submitted by fax or e-mail.
For more information and application forms, please contact: ALERT Training Division, P.O. Box 165, Addis Ababa, Ethiopia. Tel: 251-1-711524 or 712792; Fax: 251-1-711199 or 711390; email: ALERT@telecom.net.et
France. Prix "Paul Laviron. " Le prix Paul Laviron est attribué par l'Institut de Médecine Tropicale du Service de Santé des Armées. Ce prix est destiné à récompenser des travaux sur la lèpre, sa connaissance, sa thérapeutique, son contrôle. Ces travaux devront être substantiels et originaux. Ce seront des travaux non publiés, ou des travaux publiés depuis moins de cinq ans. Le montant est de 10 000 FF.
Les candidatures et une présentation des travaux, accompagnée des documents correspondants doivent être adressées au: Médecin-Général-Inspecteur, Directeur de l'Institut de Médecine Tropicale du Service de Santé des Armées, Parc du Pharo, B.P. 46, 13998 Marseille-Armées, France. - Bull. ALLF 6 (2000) 57
France. XXII Congrès Raoul Follereau. Le XXIL"'C congrès Raoul Follereau s'est déroulé à Paray-le-Monial les 25 et 26 septembre 1999, sous la présidence de M. Michel Récipon. Le compte rendu détaillé des différentes manifestations de ce congrès très réussi, peut être consulté dans le nº 321 (octobre 1999) da la revus "Lèpres."
Au plan scientifique, comme les années précédentes, le point a été fait pour les congressistes, sur la situation de la lèpre (Pr. J. Grosset) et de l'ulcère de Buruli (Pr. Carbon-Nelle). Un temps fort a été la conférence du Pr. S. Cole au cours de laquelle ce chercheur de l'Institut Pasteur, a su trouver les mots simples pour expliquer à son auditoire les résultats de ses travaux sur le génome de M. leprae (voir, dans ce même numéro du Ballf, l'interview du Pr. S. Cole que nous avons réalisé).
Les participants ont également écouté avec beaucoup d'intérêt les témoignages parfois poignants, des personnes qui sur le terrain, dans des conditions parfois difficiles, se battent pour fair reculer la lèpre et l'ulcère de Buruli.
Comme l'a dit Maurice Druon, secrétaire perpétuel de l'Académie Française, dans son discours, lu par son directeur de cabinet, lors de la remise du Prix Raoul Follereau de l'Académie Française: "Et aujourd'hui, grâce à vous, ce n'est plus le lépreux qui est repoussé, c'est la lèpre." - Bull. ALLF 6 (2000) 39
India. ILA Regional Conference of Leprosy Workers. Hind Kusht Nivaran Sangh, Maharashtra Branch, has been organizing regional conferences of leprosy workers in Maharashtra for the last several years. This has been with the primary objective of providing opportunities to grass-root-level workers to express their views and actual field experiences. This year, two regional conferences were organized: 1) Western Maharashtra region (Dist. Satara, Sangli, Kolhapur and Ratnagiri) at Richardson Leprosy Hospital, Miraj, on 11 and 12 March 2000 and 2) Kokan region (Dist. Mumbai, Thane, Raigad and Sindudurg) at Kushtarog Nivaran Samiti, Cantina, Painful, on 14 and 15 March 2000. Both conferences were dedicated to the memory of pioneering efforts of the late Shri S. S. Naik, past secretary, Hind Kusht Nivaran Sangh, Maharashtra Branch, in starting this event for leprosy workers.
Over 150 field workers from government and NGOs participated in the conferences and presented 58 papers (25 papers at Miraj and 33 at Cantina) on various aspects of leprosy: epidemiology, clinical aspects, MLEC, rehabilitation and social aspects, etc.
The conferences at Miraj and at Cantina were inaugurated by Shri Patil, Mayor of Sangli and by Shri Chandrashekhar Dhar- madhikari, Ex. Chief Justice, respectively.
The highlights of paper material, discussion and the suggestions in both the conferences were as follows:
1) The papers based on case detection in special groups of population like fishermen, prisoners, tribal population, commercial sex workers, etc., showed significantly high N.C.D.R. Hence, it was suggested to include these groups in routine surveys.
2) The results of last three MLECs in Maharashtra showed decline in new case registration. However, the experience with VRCs, this was encouraging.
3) Since the routine surveys do not reveal smear positive cases, it was suggested to make special efforts to get the hidden smear positive cases.
4) In case of smear positive cases, along with the household contacts, the contacts at the work place, travel and at social activities should also be examined.
5) If properly trained, it was expressed that leprosy patients can also disseminate information on leprosy.
6) In the conference, information on various rehabilitation schemes for leprosy patients was made available to the field workers for future reference.
7) To solve the problem of duplication of registration and to trace the drop-out cases who leave the area, it was suggested to create a state level central registry of leprosy patients.
8) All the field workers expressed that the integration of leprosy services into the general health services should be made only after proper training and motivation of general health workers.
In both conferences, field workers participated in the deliberations with keen interest and expressed their views and experiences freely.
For the benefit of field workers, the guest lectures of resource persons were arranged on the following different topics:
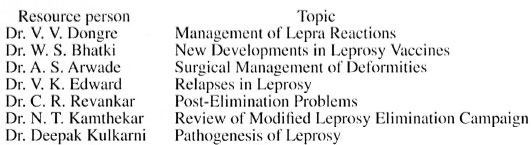
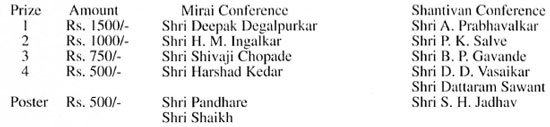
To encourage participants, the cash prizes were awarded for the best presentations in memory of the late Shri Sharad Naik:
Dr. Ponniah, Dr. R. Ganapati, Dr. Revankar, Dr. Bhatki, Dr. Dongre, Dr. Pillai, Dr. Kamthekar, Dr. Arwade, Dr. (Mr. & Mrs.) Edwards, and Dr. Deepak Kulkarni were present at the conference as experts. The efforts taken by Shri Uday Thakar, Secretary, HKNS, Mah. Br., and Smt. Pratibha Kathe, Project Co-ordinator, RRE Society, in organizing these conferences were highly appreciated by the experts and the participants. The Indian Leprosy Foundation, Mumbai, and Lepra India have substantially contributed and sponsored these conferences.
Reported by Mr. Uday Thakar, Secretary, Hind Kusht Ni varan Sangh, Maharashtra Branch, Mumbai. - Materials from U. H. Thakar, Hon. Secretary, HKNS-MB
India. 21st Biennial Conference of 1AL held at Chandigarh. The 21st Biennial Conference of the IAL was held at the Postgraduate Institute of Medical Education and Research during 17-19 September 1999 under the warm hospitality of Professor Bhushan Kumar, Department of Dermatology, STD and Leprology. More than 300 delegates, both from India and abroad, participated in the 3-day scientific conference.
On the morning of 17 September there was a symposium on the Continuing Priorities in Leprosy. The session started with a discussion on neuritis. The aim of taking this subject was to standardize live important aspects of neuritis. As a teamwork exercise, a group of experts under the chairmanship of N. B. B. Reddy framed the definitions related to neuritis; the CLT&RI, under the guidance of P. K. Oommen, identified the minimum information on structure and function of nerve; the Central JALMA Institute for Leprosy worked on the examination protocol, with B. K. Girdhar in the chair; Bombay Leprosy Project under the guidance of R. Ganapati prepared the recording and reporting system and R. S. Misra and his team finalized the management strategy. The proposed recommendations were briefly presented in the conference under the chairmanship of G. Ramu and suggestions from the delegates were incorporated. This was followed by a presentation by Diana Lockwood, the lead speaker on the subject. In her presentation she emphasized the need for a robust testing method for detecting nerve involvement early, understand the pathogenesis with reference to molecular/immunological mechanisms, and role of steroids and newer im- munomodulating agents in management of neuritis. K. V. Desikan spoke on post-MDT monitoring and evaluation and emphasized the need for an inbuilt system for surveillance to detect relapse. He also briefly dealt with the importance of justifying the utility, safety, cost-effectiveness and advantages of FDT. Ebenezer Daniel stressed the need for incorporating comprehensive eye care in the program. Ben Naaf's talk dealt with all components of reaction in brief, with paramount reference to neuritis. Indira Nath's presentation emphasized the strong probability of dysregulation of IL-4 as a major factor in bringing the clinical changes in reactions. A. N. Chakravarti's presentation emphasized the homology of animal, human and soil-derived CAN bacteria, whose genetic heterogeneity may help in evaluating the time and place of origin of the disease.
The post-lunch session had the CME under the banner 'Newer Frontiers' in which N. S. Dharmashanktu highlighted the achievements of NLEP in India, and opined that probably the program is at its peak and ripe for integration. A. M. Dhople spoke on leprosy research beyond the year 2000 A.D. while K. Prabhakaran dealt with treatment of patients relapsing after MDT. G. P. Talwar stressed the role of combined chemotherapy and immunotherapy in leprosy elimination. Yasin Quabati from Yemen projected his country's and global achievements through MDT. M. D. Gupte presented data on the comparative vaccine trial and highlighted the role of vaccines in the control of leprosy. S. K. Satpathy and B. L. Sharma presented innovative approaches of involving the community in the leprosy control program undertaken by the DANLEP.
The conference was inaugurated by Professor N. K. Ganguly, Director-General, Indian Council of Medical Research. In the inaugural session, two small books on leprosy were released and A. R. K. Pillai, Director, Indian Leprosy Foundation, was congratulated. After the inauguration, the keynote address 'A World Without Leprosy - what it should mean' was delivered by Yo Yuasa, President of ILA, and S. K. Noordeen chaired the session.
The conference received a total of 147 abstracts, of which 59 were selected for free papers and the remaining 88 were posters. The sessions for free papers were on clinical leprosy, therapy of leprosy, immunology, experimental leprosy, microbiology and pathology, and social aspects of epidemiology. These sessions were chaired by V. B. Jadhav, V. K. Sharma, S. G. Dastidar, V. P. Shetty, K.V. Desikan, Mathura Prasad, C. S. Walter, V. V. Dongre and Adarsh Chopra. There were also a couple of awards. The Acworth Research Society Award for the best paper went to Arup De Sarkar of Chandigarh. The award for the best publication went to Gigi Ebenezer, Ka- rigiri. Vishwanath Prasad, Kiran Katoch and P. B. Ranganatha Rao, respectively, received the first, second and third prizes for posters.
The valedictory session was presented by C. S. Walter, Director of the Leprosy Mission, South-East Asia. In this brief parting session, the IAL congratulated The Leprosy Mission on its completion of 125 years of dedicated service. In addition, the chairman thanked the organizing committee on behalf of the delegates and the organizing secretary thanked his team. Judged in terms of scientific content, floor management and the hospitality for the delegates, it was a superbly organized meeting. Professor Bhusha Kumar and the team he led deserve high commendation. - Lepr. Rev.
Spain. International Course for Leprosy Physicians to be held in Valencia. An International Course for Physicians will be held 24-28 October 2000 at Generalidad Valenciana and General Hospital of Valencia's Regional Government. Directed by Dr. Jose Terencio de las Aguas, the course is directed basically at Doctors/Residents in the 3rd year of Dermatology specialization, dermatologists in endemic areas of Latin America and other endemic countries, as well as licensed Medical Doctors or specialists with an affiliation with leprosy. Space is limited. For details and to enroll contact: Dr. Terencio de las Aguas by phone (34-609-605322), fax (34-966-42-3353) or email (drjoseterencio@hotmail.com).
U.K. Discovering the history of leprosy. The following article by Zoe Heming on the Global Project on the History of Leprosy appeared in the ILEP Connection.
"As the world of antileprosy work changes ever more rapidly, it is important that the history of the disease is not lost. The International Leprosy Association has recently received funding for a 3-year project known as the Global Project on the History of Leprosy. Ex-ILEP General Secretary, Paul Sommerfeld, with project assistant Zoë Heming, began the project in September. The project is intended to provide a pathway for future researchers to learn from something that has been part of human existence as far back as can be traced. The four main project areas are: identifying and linking historical resources; developing advice on maintaining records and resources for the future; video testimonies; compiling information on discriminatory legislation and customs.
"A website has been created at www.leprosyhistory.org where a data base of resources worldwide will be held. Progress and news will also be posted on the site as the project develops. We are looking for information about:
- Libraries, book collections, bibliographies
- Medical records
- Collections of personal testimonies
- Hospitals
- Private collections
- Collections of photographs/paintings
- Stamps and coinage
- Museums
- Maps
- Leprosaria
- Churches
- Organization archives
- Any other historical resources
We will be writing to ILEP Members shortly for their support in getting the word out about the project to others in the leprosy world. We look forward to your collaboration on this valuable and exciting project." - ILEP Connection 4 (Dec. 1999/Jan. 2000)3
U.S.A. Elimination of leprosy in the Americas. Two conferences on the elimination of leprosy in the Region of the Americas and in the world took place during the month of November 1999. The Third PAHO/WHO Regional Conference on the Elimination of Leprosy from the Americas was held in Caracas, Venezuela, from 3 to 5 November, in order to define a plan of action for the Region of the Americas. Convened by WHO from 15 to 17 November, the Third International Conference for the Elimination of Leprosy took place in Abidjan, Ivory Coast, and led to the announcement of the "Global Alliance to Eliminate Leprosy as a Public Health Problem in every country by the year 2005." This initiative will give the effort against leprosy its final impulse.
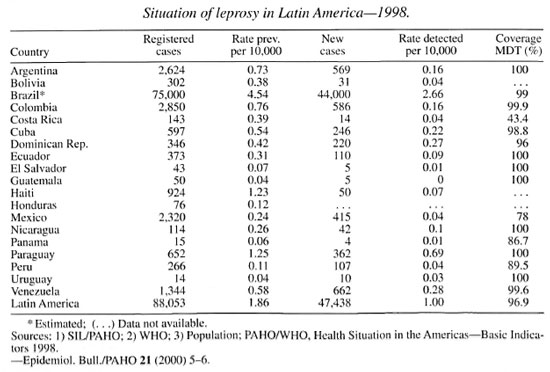
The implementation of multidrug therapy (MDT) has dramatically changed the epidemiological situation of leprosy in the Region of the Americas. The number of registered cases decreased from 369,846 in 1992 to 88,053 in 1999, while the detection rate per 10,000 population slightly increased at the regional level in the same period, with important progress in some countries, such as Brazil. The geometrical mean of the annual decrease of the prevalence rate, now at the level of 18.7%, also reflects a decrease in the number of countries where leprosy is a public health problem, from 14 to 2 in Latin America1 (Brazil and Paraguay), and from 27 to 3 in the American continent as a whole.
The elimination of leprosy from the Americas by the year 2000, through a decrease of the prevalence rate to a level below 1 case per 10,000 population, is a reachable goal that involves a reduction in the current number of registered cases of less than 10% in most countries. In the case of Brazil, where the reduction from 75,000 to 16,000 registered cases is more significant, leprosy could be eliminated within 3 to 4 years.
The countries of the American Region can be classified into the five following groups, based on different levels of priority and according to criteria such as prevalence rate, absolute number of registered cases and newly detected cases in 1998:
- Group 1: Brazil. This country is a top priority since it represents between 80% and 90% of the total burden of leprosy in the continent. Consequently, special and intensified efforts will be required to eliminate the disease through the active involvement of municipalities.
- Group 2: Paraguay and Suriname. Neither country has eliminated leprosy at the national level, but both present less than 1000 registered cases, and initiatives to accelerate the elimination of leprosy should be put in place in these countries.
- Group 3: Argentina, Colombia, Mexico and Venezuela. These countries have already eliminated leprosy at the national level, but still present over 1000 registered cases.
- Group 4: Cuba and the Dominican Republic. Both have eliminated leprosy at the national level and have less than 1000 registered cases, but more than 200 new cases were detected in 1998.
- Group 5: Other countries of the Region, with the exception of Chile (where leprosy is not endemic), the English-speaking Caribbean islands, Canada and the United States of America. These countries present more favorable official indicators. Some Central American countries had achieved elimination before MDT was implemented. In the other countries, difficulties with the information systems require detailed validation of the official data.
In the case of Latin America, due to the socioeconomic situation and some characteristics of the national health systems, it is reasonable to suspect that the elimination programs did not detect all of the existing cases in the area. Consequently, a hidden prevalence could exist, which can be estimated from the characteristics of the newly detected cases. Its importance was characterized in the following study, which includes some countries of Latin America only, due to the lack of data for the other countries.
In a group of nine Latin American countries2 representing around 80% of the population and of the leprosy prevalence in all the countries where leprosy was eliminated at the national level, the hidden prevalence was estimated at 5000 cases. From this figure, it can be estimated that there are about 7000 unknown cases in Latin American countries that have already eliminated leprosy, i.e., excluding Brazil and Paraguay.
In order to emphasize the importance and priority of the leprosy problem in areas where the elimination at the national level has already occurred, another group of eight Latin American countries3 where leprosy was eliminated was considered. Again, this sample included 80% of the population and of the leprosy prevalence in all the countries with eliminated leprosy at the national level. In these countries, approximately 30 million people live in the territories of the first sub-national level (state, province or department) where leprosy has not been eliminated. Thus, we can estimate that about 40 million people live in areas where leprosy is still a public health problem, in countries of Latin America where leprosy is considered to be eliminated at the national level. Further, of the 191 entities forming the first sub-national level, 37 (19%) have not eliminated leprosy.
Therefore, elimination strategies should be sustained even when a given country has reached elimination of leprosy at the national level. Two steps are involved in the integrated approach to insure political commitment and technical cooperation:
- The first step is confirmation, with prevalence as an indicator. In the confirmation stage, entities are classified according to their respective estimated prevalence rate and different strategies are put in place in order to evaluate hidden prevalence. Once the search and evaluation of the hidden prevalence are achieved, if it is confirmed that the prevalence is below 1 case per 10,000 population, other strategies will be implemented in order to confirm this "status," using detection (incidence) as an indicator through the promotion of community awareness and training of local health teams.
- At a later stage, when no case is detected after a 5-year period, the progressive introduction of an epidemiological surveillance system adequate for a low-prevalence scenario is proposed, using tools such as sentinel surveillance and zero reporting, until the interruption of transmission is reached, which means that the area is no longer endemic for leprosy.
The "Global Alliance" proposed the following key strategies for the 2000-2006 period: 1 ) implement the diagnosis and treatment of leprosy in all the services of the endemic area; 2) guarantee the availability of free MDT treatment in health centers through appropriate logistics; 3) motivate people to ask for treatment, through creative and higher quality interventions, to spread the information on signs and symptoms of the disease; 4) ensure high healing indices through the introduction of innovative and flexible systems of administration of MDT; and 5) monitor actively the situation to adopt appropriate actions to solve the detected problems rapidly.
In order to accelerate progress toward elimination of leprosy in Brazil, Paraguay and Suriname and to build innovative strategies to validate and consolidate the results obtained in the other countries, a proactive and sustained effort is proposed through the implementation of a Regional Plan coordinated by PAHO/WHO. As agreed during the Venezuela conference, this action plan will be elaborated in 2000. From the time of its formulation, it should count on the full commitment of a wide spectrum of partners, and a close collaboration between health care providers and users at every level of leprosy care. The objectives of the Regional Plan should be to prevent the re-emergence of the disease as well as, through the use of new technologies, the total interruption of its transmission, i.e., the eradication of leprosy from the Americas.
1. Latin America includes: Argentina, Bolivia, Brazil, Colombia, Costa Rica, Cuba, Dominican Republic, Ecuador, Guatemala, Haiti, Mexico, Nicaragua. Paraguay and Venezuela.
2. Argentina, Bolivia, Colombia, Cuba. Dominican Republic, Ecuador. Mexico, Peru, and Venezuela.
3. Argentina, Bolivia, Cuba. Mexico. Peru, Dominican Republic, and Venezuela.