- Volume 68 , Number 3
- Page: 258–66
Leydig cell hyperplasia and the maintenance of bone volume: bone histomorphometry and testicular histopathology in 29 male leprosy autopsy cases
ABSTRACT
This study was conducted to determine if osteoporosis in male leprosy patients is caused by testicular atrophy. Bone volume (BV/TV), trabecular number (TbN), trabecular thickness (TbTh), and trabecular separation (TbSp) were measured in two areas in decalcified paraffin sections of lumbar bones from 29 male leprosy and 6 male nonleprosy autopsy cases. We found significant differences in the average BV/TV measurements among the 7 patients with nodular Leydig cell hyperplasia (BV/TV 12.24%) and the 22 patients without hyperplasia (BV/TV 7.35%) and 6 patients without leprosy (BV/TV 12.98%). Bone volume was maintained in patients with nodular Leydig cell hyperplasia, and we determined no clinical factor other than the Leydig cell hyperplasia that reflected the bone volume. The osteoporosis of male leprosy patients was attributed to secondary gonadal dysfunction due to testicular atrophy, and Leydig cell hyperplasia appears to preserve bone volume.RÉSUMÉ
Cette étude fut mise en uvre pour savoir si l'ostéoporose chez les patients de sexe masculin est une conséquence de l'atrophie testiculaire. Le volume osseux (BV/TV), le nombre des travées (TbN), l'épaisseur des travées (TbTh), l'espace entre les travées (TbSp) furent mesurés dans deux zones à partir de sections en paraffine déminéralisées d'os des lombes de 20 cas lépreux et 6 cas non lépreux de sexe masculin. Nous trouvâmes des différences significatives des mesures moyennes de BV/TV entre les 7 patients présentant une hyperplasie nodulaire des cellules de Leydig (BV/TV = 12,24%) et les 22 patients sans hyperplasie (BV/TV = 7,35%) et les 6 patients sans lèpre (BV/TV 12,98%). Le volume osseux a été maintenu chez les patients présentant une hyperplasie nodulaire des cellules de Leydig et nous n'avons pas trouvé d'autres facteurs pouvant expliquer ce volume osseux autre que l'hyperplasie Leydigienne. L'ostéoporose des patients hanséniens de sexe masculin fut attribuée à une dysfonctions gonadique liée à l'atrophie testiculaire, et l'hyperplasie des cellules de Leydig semble permettre de préserver le volume osseux.RESUMEN
Este estúdio se realizo para determinar si la osteoporosis en los pacientes masculinos con lepra es causada por atrofia testicular. Se tomaron como muestras de autopsia, fragmentos de los huesos lumbares de 29 pacientes con lepra y de 9 personas sin lepra. Las muestras se descalcificaron y procesaron para hacer cortes en parafina y en los cortes se midieron, el volumen óseo (BV/TV), el número trabecular (TbN), el grosor trabecular (TbTh), y Ia separación trabecular (TbSp) en dos áreas. Se encontraron diferencias significativas en las mediciones promedio dei volumen óseo entre los siete pacientes con hiperpiasia nodular de Ias células de Leydig (BV/TV 7.35%) y los 6 pacientes sin lepra (BV/TV 12.98%). El volumen óseo se mantuvo en tos pacientes con hiperpiasia nodular de células de Leydig y no se encontro ningún otro factor clínico, aparte de la hiperpiasia de tas células de Leydig, que reflejara el volumen óseo. La osteoporosis de los pacientes masculinos con lepra se atribuyó a la dis función gonadal secundaria a la atrofia testicular. La hiperpiasia de las células de Leydig parece preservar el volumen óseo.Hypogonadism is a major factor in decreased bone content among males (7,8,20,22,23), and there are many men with hypogonadism that is not diagnosed until fracture (1,2). Hypogonadism is well known in male leprosy patients and is attributed to testicular damage by orchitis (14,16, 17). Reports on osteoporosis in hypogonadal leprosy patients, however, are scarce. We previously studied serum free testosterone and bone mineral density (BMD) with dualenergy Xray absorptiometry (DXA) in male leprosy patients and speculated that osteoporosis in male leprosy patients is a secondary condition caused by gonadal dysfunction (11,12).
In this study, using histopathologic and histomorphometric methods, we explored this hypothesis by comparing the degree of testicular damage to the degree of trabecular bone loss in autopsy cases. We are aware of no other study comparing the histomorphometric changes of vertebral trabecular bone to the pathologic testicular changes in cases of male leprosy.
MATERIALS AND METHODS
We used 29 male leprosy autopsy patients (54 to 79 years of age, average 66.5 years) and six agematched, male non leprosy autopsy patients as controls (52 to 69 years of age, average 61.5 years). All leprosy patients were residents of Oku KomyoEn Leprosarium, Okayama, Japan, for at least 20 years, some for as long as 50 years, and all were lepromatous, including one with active disease. The nonleprosy controls were patients at a nearby general hospital. All patients, leprosy and non leprosy, died of causes not related to conditions known to affect bone metabolism. They all died within 1 month after their final hospitalization. Cases of liver cirrhosis or diabetes mellitus were not included due to a possible association with osteoporosis. The leprosy patients had been treated with corticosteroids in periods of acute exacerbation due to other conditions. Seventeen of the 29 patients had received 10 mg to 1850 mg of corticosteroids in the form of prednisolone, including tablets, injections, ointment, or ophthalmic solution (clinical data is shown in Table 1). Gynecomastia, low body mass index (BMI) (15), difficulty with gait, or massive doses of steroids were suggestive of osteoporosis, to the point of affecting remodeling of the trabecular bone.
Testes. Testes of the patients were weighed and fixed in 10% formalin during autopsy (Table 2). They were then processed for paraffin sections and stained with hematoxylin and eosin (H&E). Three histologic patterns were seen: a) nodular Leydig cell hyperplasia (Fig. 1A) with or without sperm in the seminiferous tubules, b) total scarring (Fig. 2A), and c) no remarkable Leydig cell proliferation with or without sperm. The nodular hyperplasia pattern was prominent and more widely distributed through out the testes than were the other two patterns, although it was found in fewer patients. Since the Leydig cells secrete androgen, the tissue specimens from leprosy patients were divided into two groups according to the degree of nodular hyperplasia of the Leydig cells. The first group showed remarkable nodular hyperplasia of the Leydig cells (hyperplasia group, N = 7) (Fig. 1A); the other group was without nodular hyperplasia of the Leydig cells (nonhyperplasia group, N = 22). The latter group included patients with totally scarred testes. We determined testicular atrophy by testicular weight and histology, including evidence of atrophy of the seminiferous tubules. Scarring and scant sperm were also considered evidence of atrophy. Table 2 shows the pathological findings. Pituitary glands of four patients (Cases 16, 23, 25, 26) were also examined histologically to check for hyperplasia of the basophilic cells which secrete interstitial cellstimulating hormone, resulting in Leydig cell hyperplasia.
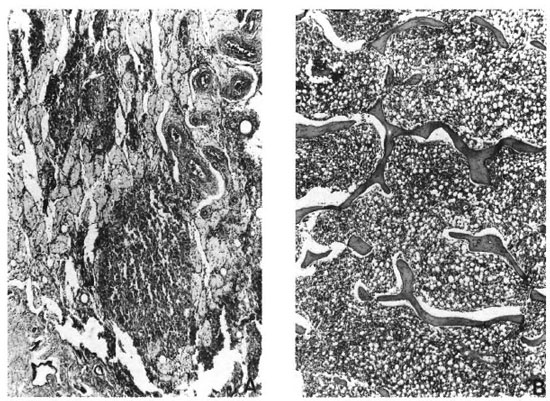
Fig. 1. Microscopy findings of testis and vertebral bone in leprosy patients with Leydig cell hyperplasia. A= Testis (H&Ex20); nodular Leydig cell hyperplasia with scarry stroma. B = Vertebral bone (H&E x40); bonetrabeculae are thick and mostly continuous. Average BV/TV is 12.24%.
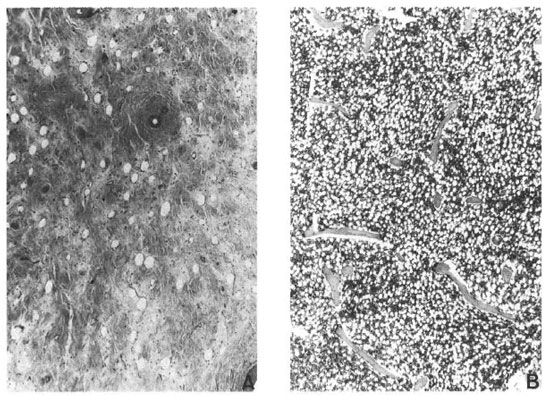
Fig. 2. Microscopy findings of testis and vertebral bone in nonLeydig cell hyperplasia leprosy patients. A =Testis (H&E x20); scarry testis; no Leydig cells or seminiferous tubules are evident. B = Vertebral bone (H&Ex40); thin and perforated trabeculae are present. Average BV/TV is 7.35%.
Vertebral bone. Bone specimens from the 2nd or 3rd lumbar vertebral bones intheir frontal plane were decalcified, processed for paraffin sections, and stained with H&E. Each histological section of bone was photographed at low magnification (x20) in two areas, near the cortex (Ct area) and from the center of the body of the bone (Cn area). The thickness of bone trabecule of the leprosy patients varied from thin to thick, as shown in Figures 1B and 2B. Thin trabeculae showed remarkable perforation or discontinuity (Fig. 2B). Thin, scanty trabeculae with perforation is considered histologic evidence of osteoporosis. The bone of nonleprosy patients showed thick, continuous, abundant trabeculae (Fig. 3B). Bone in the hyperplasia group was characterized by thick, continuous, abundant trabeculae similar to that of the non leprosy patients.
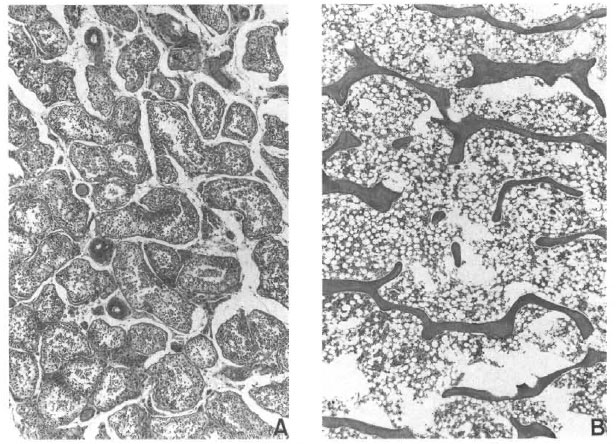
Fig. 3. Microscopy findings of testis and vertebral bone in nonleprosy control patients. A = Testis (H&Ex20); small aggregates of Leydig cell and seminiferous tubules with sperm were normal. B = Vertebral bone(H&Ex40); thick continuous spiculae are present. Average BV/TV is 12.98%.
Measurement. Using the photographsof trabecular bone, we measured the bone medullary bone (BV/TV), the trabecular thickness (TbTh), the trabecular number (TbN), and the trabecular separation (TbSp) in both areas (18, l9). We compared BV/TV, TbTh, TbN, and TbSp among the hyperplasia, nonhyperplasia, and control groups. A low BV/TV, markedly reduced TbTh, few TbN, and pronounced TbSp indicate osteoporosis. Age matching was done among the three groups, and the data are shown in Table 2.
Analysis. Analysis of the trabecular structure was performed on a Macintosh computer using the public domain NIH image program written by Wayne Rasband, which can be obtained as freeware from http://rsb.info.nih.gov/nihimage/index.html. Statistical analyses were performed with StatView 4.5 (Abacus Concepts Inc., Berkeley, California, U.S.A.). All values are expressed as mean ± S.D. unless otherwise indicated. Statistical differences among groups were evaluated with the KruskalWallis test or MannWhitney test. The relationship between pairs of variables was assessed by Spearman rank correlation analysis; p values of <0.05 were considered statistically significant.
RESULTS
Analysis of trabecular structure. The differences in BV/TV, TbTh, TbN, and TbSp among the hyperplasia, nonhyperplasia, and control groups are shown in Table 3. Significant differences were observed in the average measurements of BV/TV at Ct, TbTh at Ct and Cn, TbN at Ct, and TbSp at Ct among the hyperplasia, nonhyperplasia, and control groups (Table 3; Fig. 4). At Ct, BV/TV, TbTh, and TbN in the hyperplasia group matched those of the controls, and TbSp also matched that of the controls. At Cn, only TbTh differed; it was significantly decreased in the hyperplasia group. Testicular weight was significantly lower in the leprosy patient groups than it was in the controls. No significant differences in age at death, BMI, BV/TV at Cn, TbN at Cn or TbSp at Cn were found. Age at onset of leprosy, age at death, BMI, steroid usage, and testis weight showed no significant correlation with the BV/TV at Ct (Table 4). Comparison of BV/TV between patients with testicular atrophy or steroid use and those without either of these clinical factors revealed no significant differences. There were too few cases to compare them statistically with respect to vasectomy, gynecomastia, or gait instability. However, all three patients with gynecomastia (Cases 8, 21, and 22) showed nodular Leydig cell hyperplasia.
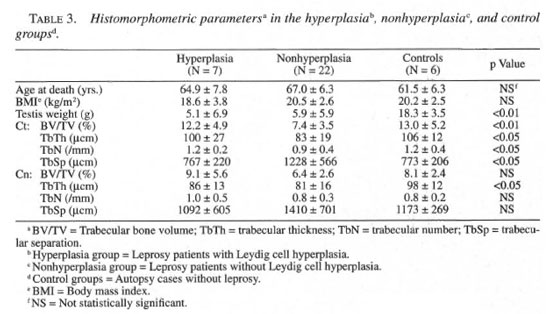
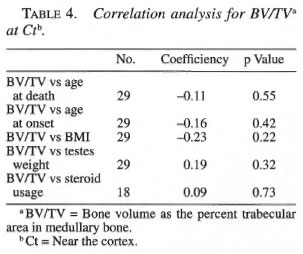
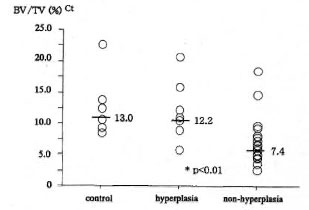
FIG. 4. Correlation analysis for BV/TV near thecortex (Ct) in the hyperplasia, nonhyperplasia, andcontrol groups.
Pathology of testes. The weight of the testes of the leprosy patients ranged from 2.0 g to 20.5 g (average 5.73 g), and that of the control patients ranged from 13.0 g to 22.0 g (average 18.3 g) (Table 2). Testicular atrophy of the leprosy patients was remarkable, and the difference between the leprosy patients and the control patients was significant (p <0.001) (Table 3).
Microscopically, testicular scarring was evident in all leprosy cases, i.e., in both the hyperplasia and nonhyperplasia patients, but it varied widely from totally fibrotic (Fig. 2A) to largely normal with focal scarring. The testes of 24 leprosy patients showed seminiferous tubules in varying numbers, but five of these patients showed no tubules within scarred tissue (Cases 13, 15, 16, 22, 24). There were no significant differences in BV/TV between cases of totally scarred testicular atrophy and cases of nonscarring. Nodular Leydig cell hyperplasia was prominent in the hyperplasia group (Fig. 1A). Immunohistochemically, using the avidinbiotin peroxidase complex (ABC) method, testosterone was positively stained in hyperplastic Leydig cells (Fig. 5), showing that hyperplastic Leydig cells secrete testosterone. Spermatozoa were present in the testicular tubules of 10 leprosy patients; the other 19 showed no sperm within the atrophied tubules or totally scarred testes. There were no significant differences in BV/TV between patients with and without sperm. Histologically, the four pituitary glands studied (Cases 16, 23, 25, 26) showed no hyperplasia of the basophilic cells which secrete interstitial cell (Leydig cell) stimulating hormone.
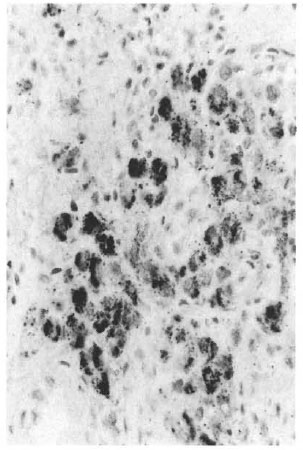
Fig. 5. Immunohistochemical staining of hyperplasic Leydig cells in testicular tissue from the hyperplasia group. Note that testosterone is clearly positive (ABCx400).
DISCUSSION
Only a few studies have analyzed the histomorphometry at the iliac bone in men (35, 13), and only Jackson, et al. reported bone histomorphometry in hypogonadal men (13). None of these studies gave pathological descriptions of testicular atrophy. According to our data, BV/TV, TbTh, TbN, and TbSp all differed significantly at Ct between the types of patients; however, at Cn, only TbTh differed. The Ct area tended to be more sensitive to hormonal change than did the Cn area. BV/TV at Ct in the nonhyperplasia group was significantly less than that in the control group. TbTh at Ct and Cn and TbN at Ct in the nonhyperplasia group were significantly less than those in the control group, and TbSp at Ct was significantly greater. Chappard, et al. reported that bone trabecular perforation in corticosteroid therapy patients occurred when BV/TV was less than 11 % (3). In their study, the bone biopsy was of the iliac crest and undecalcified sections were used. Our method differed from theirs, but our findings agreed. In our nonhyperplasia group, TbTh was reduced to 100 jam and perforation occurred, so TbSp was greater and BV/TV was reduced to below 11%. However, it is difficult to explain how BV/TV, TbTh, TbSp, and TbN were maintained in the hyperplasia group comparable with those of the control group. Did perforation not occur in the hyperplasia group due to protection from bone spicular erosion?
Testicular weight was significantly lower in the leprosy patient groups than it was in the controls. This is explained by the postinflammatory damage of testes of leprosy patients. However, testicular weight did not correlate with B V/TV in our 29 leprosy patients. Leydig cell: eusecreted hormones may regulate the volume of trabecular bone, and Leydig cell status rather than testicular weight may be the important factor influencing bone volume. In other words, Leydig cell hyperplasia may protect from osteoporosis in leprosy patients with testicular damage.
No significant correlation was found between BV/TV at Ct and other clinical factors (age at disease onset, age at death, BMI, and the steroid hormone therapy) that might cause the BV/TV to decrease. If testosterone production is significantly reduced in leprosy patients in their younger years, bone loss would resemble that of menopausal women.
We conclude that the osteoporosis of male leprosy patients is caused by secondary gonadal dysfunction. Our findings may contribute to understanding the pathogenesis of osteoporosis in male leprosy patients and should support the development of hormone therapy for leprosy patients as well as hypogonadal patients without leprosy (6,9,10,21,24).
Acknowledgment. We thank Professor T. Naka mura and Dr. H. Tsurugami, School of Medicine, University of Occupational and Environmental Health, and Assistant Professor K. Yoh, Hyogo College of Medicine, for advice regarding histomorphometric methods.
REFERENCES
1. Baillie, S. P., Davison, C. E., Johnson, F. J. and Francis, R. M. Pathogenesis of vertebral crush fracture in men. Age Ageing 21(1992)139141.
2. Bridges, A. B., Davies, R. R. and Espley, A. J. Male hypogonadism presenting as back pain secondary to osteoporosis. Scott. Med. J. 35(1990)178179.
3. Chappard, D., Legrand, E., Basle, M. F., Fromont, P.. Racineux, J. L.. Rebel, A. and Audran, M. Altered trabecular architecture induced by corticosteroids: a bone histomorphometric study. J. Bone Miner. Res. 11(1996)676685.
4. Compston, J. E., Mellish, R. W. E., Croucher, P., Newcombe, R. and Garrahan, N. J. Structural mechanisms of trabecular bone loss in man. J. Bone Miner. Res. 6(1989)339350.
5. Delichatsios, H. K., Lane, J. M. and Rivlin, R. S. Bone histomorphometry in men with spinal osteoporosis. Calcif. Tissue Int. 56(1995)359363,
6. Devogelaer, J. P., De Cooman, S. and De Deux chaisnes, C. N. Low bone mass in hypogonadal males. Effect of testosterone substitution therapy, a densitometric study. Maturitas 15(1992)1723.
7. Finkelstein, J.S., Klibanski, A., Neer, R.M., Greenspan, S. L., Rosenthal, D. I. and Crowley, W. F., Jr. Osteoporosis in men with idiopathic hypogonadotropic hypogonadism. Ann. Intern. Med. 106(1987)354361.
8. Foresta, C., Ruzza, G., Mioni, R., Guarneri, G., Gribaldon, R., Meneghello, A. and Mastrogla como, I. Osteoporosis and decline of gonadal function in the elderly male. Horm. Res. 19(1984)1822.
9. Foresta, C., Zanatta, G. P., Busnardo, B., Scanelli, G, and Scandellari, C. Testosterone and calcitonin plasma levels in hypogonadal osteoporotic young men. J. Endocrinol. Invest. 8(1985) 377379.
10. Greenspan, S. L., Oppenheim, D. S. and Klibanski, A. Importance of gonadal steroids to bone mass in men with hyperprolactinemic hypogonadism. Ann. Intern. Med. 110(1989) 526531.
11. Ishikawa, S., Ishikawa, A., Yoh, K., Tanaka, H. and Fujiwara, M. Osteoporosis in male and female leprosy patients. Calcif. Tissue Int. 64(1999)144147.
12. Ishikawa, S., Tanaka, H., Mizushima, M., Hashizume, H., Ishida, Y. and Inoue, H. Osteoporosis due to testicular atrophy in male leprosy patients. Acta Med. Okayama 51(1997)279283.
13. Jackson, J. A., Kleerekoper, M., Parfit, A. M., Rao, D. S., Villanueva, A. R. and Frame, B. Bone histomorphometry in hypogonadal and eugonadal men with spinal osteoporosis. J. Clin. Endocrinol. Metab. 65(1987)5358.
14. Job, C. K. Gynecomastia and leprous orchitis; a preliminary study. Int. J. Lepr. 29(1961)423141.
15. Kin, K., Kushida, K., Yamazaki, K., Okamoto, S. and Inoue, T, Bone mineral density of the spine in normal Japanese subjects using dualenergy Xray absorptiometry: effect of obesity and menopausal status. Calcif. Tissue Int. 49(1991)101106.
16. Martin, F. I. R., Maddocks, I., Brown, J. B. and Hudson, B. Leprous endocrinopathy. Lancet 21(1968)13201321.
17. Morley, J. E., Distiller, L. A., Sagel, J,, Kok, S. H., Kak, G., Carr, P. and Katz, M. Hormonal changes associated with testicular atrophy and gynaecomastia in patients with leprosy. Clin. Endocrinol. 6(1977)299303.
18. Parfitt, A. M., Drezner, M. K., Glorieux, F. H., Kanis, J. A., Malluche, H., Meunier, P. J., Ott, S. M. and Recker, R. P. Bone histomorphometry: standardization of nomenclature, symbols, and units. J. Bone Miner. Res. 2(1987)595610.
19. Parfitt, A. M., Mathews, C. H. E., Villanueva, A. R., Kleerekoper, M., Frame, B. and Rao, D. S. Relationships between surface, volume, and thickness of iliac trabecular bone in aging and in osteoporosis. J. Clin. Invest. 72(1983)13961409.
20. Stanley, H. L., Schmitt, B. P., Poses, R. M. and Deiss, W. P. Does hypogonadism contribute to the occurrence of a minimal trauma hip fracture in elderly men? J. Am. Geriatr. Soc. 39(1991)766771.
21. Tenover, J. S. Effects of testosterone supplementation in the aging male. J. Clin. Endocrinol. Metab. 75(1992)10921098.
22. Vanderschueren, D. and Bouillon, R. Androgens and bone. Calcif. Tissue Int. 56(1995)341346.
23. Van der Weref ten Bosch, J. J. and Bot, A. Some skeletal dimensions of males with isolated gonadotrophin deficiency. Neth. J. Med. 41(1992)259263.
24. Young, N. R., Baker, H. W. G., Liu, G. and See man, E. Body composition and muscle strength in healthy men receiving testosterone enanthate for contraception. J. Clin. Endocrinol. Metab. 77(1993)10281032.
1. M.D., Ph.D., Department of Rehabilitation, Higashi Osaka Hospital, 1722 Chuo, Jotoku,Osaka 5360005, Japan.
2. M.D., Ph.D., Department of Pathology, Gifu Prefectural Tajimi Hospital, Tajimi, Japan.
3. M.D., Ph.D., Department of Pathology, National Leprosarium Oku KomyoEn, Okayama, Japan.
4. M.D., Department of Anesthesiology, National Leprosarium Nagashima AiseiEn, Okayama, Japan.
5. M.D., Ph.D., Department of Physical Therapy, Schoolof Health Science, Kibi International University, Takahashi, Japan.
Reprint requests to Dr. Satoshi Ishikawa at the above address or FAX 81669397474; email: wisdom99@kcc.zaq.ne.jp
Received for publication on 16 September 1999.
Accepted for publication in revised form on 7 June 2000.