- Volume 66 , Number 1
- Page: 34–42
Dietary habits, food intake and functional outcomes in those with a history of hansen's disease in Korea
ABSTRACT
This study shows that the nutrition and health status of ex-leprosy patients in Korea was marginal. Their nutrient intakes were low, especially f rom micronutrients which were associated with food f rom animal sources. Dietary quality was discriminated by food habits, such as skipping meals, irregularity of meals, food purchase and meal preparation. Dietary quality was best predicted by food habits followed by physical fitness and nutrition knowledge. Our subjects were nutrition-conscious, but they did not have accurate information. These findings suggest that our study population needs nutrition education.RÉSUMÉ
Cette étude montre que l'état nutritionnel et sanitaire des anciens malades de la lèpre était déficient en Corée. Les apports en nutriments étaient faibles, particulièrement en nutriments associés à des nourritures d'origine animale. La qualité diététique était influencée par des habitudes alimentaires telles que des sauts de repas, l'irrégularité des repas, l'achat de nourriture et la préparation des repas. Les meilleurs prédicteurs de la qualité diététique étaient les habitudes alimentaires, suivies de la condition physique et des connaissances en matière de nutrition. Nos sujets avaient conscience de l'importance de la nutrition, mais ne disposaient pas d'informations précises. Ces observations suggèrent que notre population d'étude a besoin d'une éducation nutritionnelle.RESUMEN
Este estudio muestra que la nutrición y el estado de salud de los ex-pacientes con lepra en Corea fueron marginales. Sus consumos de nutrientes fueron bajos, especialmente en micronutrientes de origen animal. La calidad de la dieta fue inapropiada debido a circunstancias tales como el ayuno voluntario o forzado, la irregularidad en las comidas, la incapacidad de compra, y la mala preparación de la comida. Los hábitos alimentarios fueron mejores en personas acostumbradas a hacer ejercicio y en aquellas con cierto conocimiento sobre nutrición. Nuestros pacientes fueron conscientes de la bondad de los buenos hábitos alimentarios pero no tuvieron información adecuada sobre el tema. Estos hallazgos sugieren que nuestra población de estudio necesita educación sobre nutrición.Complex interaction between undernutrition and Hansen's disease is well reported. Undernutrition leads to impairment of immunity which has a profound impact on the entire immune system (14). Deprivation of nutrition, thus, plays an important role not only in predisposing to leprosy but also in increasing the relapse rate of leprosy (3,4). Dietary factors that are reported to influence the etiopathogenesis of leprosy are vitamins A, B group, C, D, E, iron, calcium and zinc(4).
It is estimated that there are approximately 50,000 leprosy patients in Korea (Kyunggi Province Korean Leprosy Control Association. Hansen's disease, 1986). Among them only 50% are registered patients as members of the Korean Leprosy Control Association. Patients with inactive leprosy have gathered together and settled at resettlement villages since the 1960s (7). There are 97 resettlement villages in which 8140 ex-leprosy patients reside (Chung, S.K. The future of resettlement villages in Korea. Lee, D.M. Policies on leprosy control in Korea. Both presented at the seminar of Korean Leprosy Control Association, 1994). Eighty-one percent of those villages are located in rural areas and the rest of them (19%) are in suburban areas. Regarding their means of support, two thirds of the residents of the resettlement villages are engaged in poultry and pig-raising businesses. Recently, the industry in some of the more nearly urban resettlement villages has evolved from poultry and pig raising into small-scale industry, such as manufacturing furniture and making parts for machinery. In fact, the income of the ex-leprosy patients engaged in small-scale businesses has increased, particularly for those residing in the villages near Seoul, the capital of Korea (Chung and Lee, as cited above). These resettlement villages are mostly located in Kyunggi Province. Since the economic situation of the residents in the resettlement villages has become better, a growing concern on diet and health has unfolded among them. The Kyunggi Provincial Korean Leprosy Control Association proposes to launch a social program for the residents in order to improve nutrition and health services. To provide the basis of the program, this study was conducted to assess dietary intake and the risk factors related to nutrition, which has not yet been examined.
The ex-leprosy patients have lived in the resettlement villages separated from their families as well as from mainstream society in Korea for over a quarter of a century. A growing elderly population is one of the characteristics of the resettlement villages. It is estimated that one half of the residents in those villages are over 60 years old (Chung and Lee, as cited above) which is more than five times higher than the proportion of the elderly over 60 in Korea (8.7%) (11). Inadequate nutrient intake, particularly of micronutrients, of the aging population in Korea is well recognized (8,9).
Not only leprosy patients but also those with inactive leprosy have to take antileprosy drugs for most of their lives. There is evidence that increasing age is associated with an increased magnitude of dapsone-related hemolysis (2). The evidence from the greater proportion of the older and lifetime antileprosy drug-taking patients suggests that they are a nutritionally at-risk group and that there is a need for nutrition intervention to improve their nutritional wellbeing.
This study was conducted to examine the dietary intake and limiting factors related to better nutrition among the patients with inactive leprosy from the resettlement villages in an attempt to find an appropriate means for nutrition intervention.
MATERIALS AND METHODS
Subjects and study area. This study identified 87 ex-leprosy patients (42 males and 45 females) from the three resettlement villages in Kyunggi Province (Yeuwang, Donggin, and Chungchun). The three villages were selected because representatives of these villages expressed their willingness to participate in the study. From Seoul, one can travel by bus or automobile on paved roads to the villages in approximately 1 1/2 -2 hours. Until several years ago, these ex-leprosy patients were engaged in poultry farming which recpiired strenuous physical work. More recently, many of these residents have been engaged in small-scale industry, which has led to the accumulation of wealth. One can find factories, particularly for furniture, in almost every other building in these villages. The physical environment appears not to meet the villagers' needs. They were living with the noise and odors produced by the factories. Food, however, is easily accessible from grocery stores, traditional markets and food trucks.
Field methods and materials. Information on this study was collected as part of a regular check up provided by the Kyunggi Provincial Korean Leprosy Control Association. Information on medical history was obtained from the residents' medical records. A well-trained nutrition student (either a graduate student or senior undergraduate) from Seoul National University conducted an interview with each subject. Each interview took 25-30 minutes. The information obtained included health sta s, life style, nutrition knowledge, food intake and physical fitness. The questionnaire on health status and life style included 34 items adapted from Yu's study (Yu, J.Y. Development and assessment of food frequency questionnaire estimating dietary intake of the adults in rural areas of Korea. Master's thesis, Seoul National University, 1994). The nutrition knowledge test was developed by the investigators based on the tests provided by Song(12) and the Korean Dietetic Association (Korean Dietetic Association. Nutritional management for working people, 1994). The nutrition knowledge test consisted of items that were answered either "yes," "no," or "do not know." Both accuracy and recognition scores were calculated. Out of the total, the accuracy score was the percentage of correct answers and the recognition score was the percentage of both correct and incorrect answers.
We found that subjects were reluctant to tell us their economic situation partly because their income sources were complicated or they were afraid of losing social welfare benefits. Thus, we used village type as a measure of socioeconomic status (SES) since one study village was worse off than the other two economically, according to the information from the Korean Leprosy Control Association. This was supported by our preliminary study. In the low-income village, 46% of the residents spent less than 200,000 won per month while 6%-7% of their counterparts in other villages fell under that category. Conversely, 9% of the residents in the low-income village and 53%-67% of the residents in the high-income villages spent more than 500,000 won for monthly living.
Dietary intake was assessed by a 66-item semiquantitative food frequency questionnaire. The food list and typical portion size were based on food records collected from 132 older adults from a rural area (Yu, as cited above) and the data from the national nutrition survey in Korea (Ministry of Health and Social Affairs. National nutrition survey report, 1994). Portion size was asked as part of the food item question. The food frequency questionnaire included 12 items for vegetables, 9 for fruits, 9 for fish and shellfish, 7 for drinks, 6 for meat and meat products, 5 for beans, 3 for kimchis, 3 for legumes, 3 for rice and rice cakes, 2 for noodles, 2 for seaweeds, 1 for bread, 1 for biscuits, 1 for candy, 1 for garlic, and 1 for eggs. As suggested by Willett (13), individual food values were calculated for nutrients by using the Korean food composition table (Food and Drug Administration, Ministry of Health and Social Welfare. Korean food composition table, 1996). Nutrientadequacy and mean adequacy ratios (5) were also calculated. The Nutrient Adequacy Ratio (NAR) represented an index of adequacy for a nutrient based on the corresponding Korean Recommended Daily Allowance (RDA). The Mean Adequacy Ratio (MAR), a mean of NARs of eight nutrients (energy, protein, calcium, iron, vitamin A, thiamin, riboflavin, ascorbic acid) provided an index of the overall quality of the diet.
Statistical analyses. Statistical analyses were performed using the 1994 Statistical Analysis System (SAS) 6.11 ed. The nature Borderlineof the individual variables was examined by univariate statistics. Based on the results of the descriptive analyses, some variables were reconstructed as necessary. If a variable was not normally distributed, it was transformed into log form in order to normalize the distribution. A chi-squared test was used to compare between males and females in terms of food habits and .the degree of physical fitness. Regression analyses were used to examine the relationships of the quality of diet and food habits while controlling for age and gender. Regression analyses were also performed to assess the relative strength of variables related to the due to the quality of diet. All variables used in the model were initially included on theoretical grounds. MAR was used as a response variable. Predictive variables included nutrition knowledge, food habits (frequency of skipping meals per week and regularity of eating), health status, physical fitness, socioeconomic status, gender and age.
RESULTS
General characteristics. In terms of medical history, lepromatous leprosy (81%) had the highest proportion followed by tuberculoid leprosy (15%), indeterminate leprosy (3%), and borderline leprosy (1%) (Table 1). Based on the classification of leprosy for the purpose of social rehabilitation(7), 36% of the subjects were diagnosed with Deformity I (normal appearance of normal person with normal labor capacity), , 31 % as Deformity III (definite appearance of leprosy but with moderately impaired labor capacity), and 1% as Deformity IV (advanced case of leprosy with capacity only for light work).
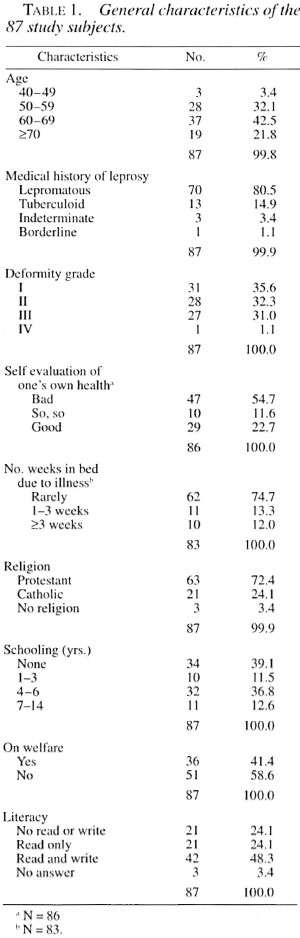
Two thirds of the subjects were over 60 years old. Approximately 40% of the subjects had never been to school. The subjects were a religious group, 72% being Protestant and 24% Catholic. Forty percent of the subjects were the recipients of social welfare programs. In terms of literacy, 50% of the subjects were able to read and write;25% were illiterate.
One third of the subjects thought that they were healthy while 54% considered themselves unhealthy (Table 1). During thepast year, 71% of the subjects rarely laysick in bed while 13% of them were ill in bed for 1-3 weeks and 12% for more than 3 weeks. Neuralgia and arthritis, found in more than 50% of the subjects, were the most frequently reported diseases, followed by gastrointestinal disorders, hypertension and diabetes.
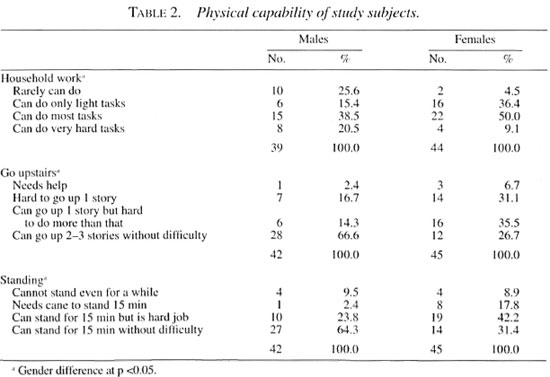
Physical fitness. For aging individuals,physical inability limits food preparation which may, in turn, prevent them from having foods they need or want. This study measured the degree of physical fitness regarding household work, ascending stairsand standing. Difficulties in performing household work, ascending stairs and standing. Difficulties in performing household work were seen in 40% of the subjects (Table 2). About one third of the subjects did not have enough physical strength to ascend stairs. For one half of them, standing for more than 15 minutes was a difficult task (Table 2). Females were physically less capable than males. Two thirds of the males were able to go up 2-3 stories and stand 15 minutes without difficulty. On the other hand, less than one third of the females were able to perform these activities.
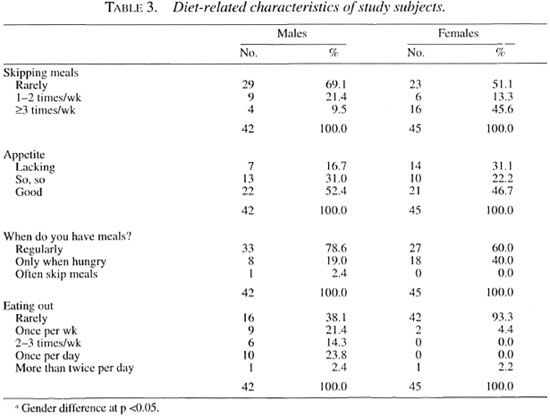
Food habits. Sixty percent of the subjects indicated that they did not skip meals (Table 3). One third of the subjects (16 females and 4 males) said they skipped meals more than three times a week, primarily due to a lack of appetite. Approximately 50% of the subjects did not have a good appetite. Compared to males, the females skipped meals more frequently and had less appetite (Table 3). Approximately 30% of the subjects had meals only when they felt hungry. Eating out was not preferred; about 80% of them rarely ate out.
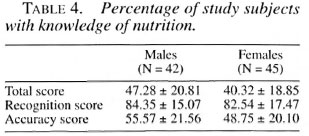
Nutrition knowledge. The study subjects recognized 84% of the total items, but correctly answered only 52% of the items that they recognized (Table 4). This suggests that they were concerned with nutrition but did not have accurate information on it. Scores on the nutrition knowledge test were independent of gender and age.
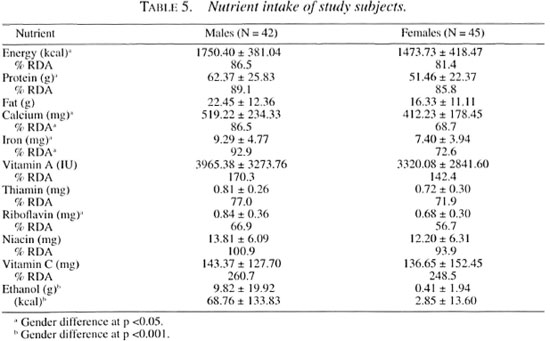
Food and nutrient intake. The subjects had rice and kimchi (pickled cabbage and radish) more than once a day. On average, they consumed 648 g of rice and 88 g of kimchi every day. The amount of rice was more than twice as much as the national mean (314 g) while that of kimchi was less than the national mean (115 g) (Ministry of Health and Social Affairs. National nutrition survey report, 1994). Foods eaten more than once a day by more than 25% of the subjects were rice, barley, bean, kimchi, onion, bean paste and coffee. This suggests that the subjects had a monotonous diet which depended largely on rice and kimchi. The mean daily energy consumptions were 1750 and 1473 kcal for males and females, respectively (Table 5). The absolute energy intake of males was higher than that of females but in terms of the percentage of the RDA, little difference was found between them (86.5% and 81.4% of the Korean RDA for males and females, respectively). Micronutrient intake was low, particularly for females. Females had 57% 73% of the RDA for thiamin, riboflavin, calcium, and iron, and consumed less calcium and iron than did the males.
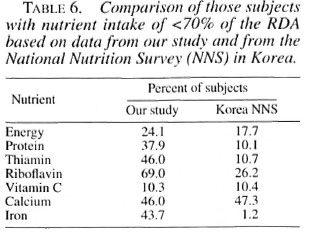
The results of our study were compared to those from a 1994 national nutrition survey in Korea (Ministry of Health and Social Affairs. National nutrition survey report,1994). The percentage of subjects with in sufficient nutrients was much higher in our study (Table 6). More than 40% of our subjects had thiamin, riboflavin, calcium and iron intake of less than 70% of the Korean RDA.
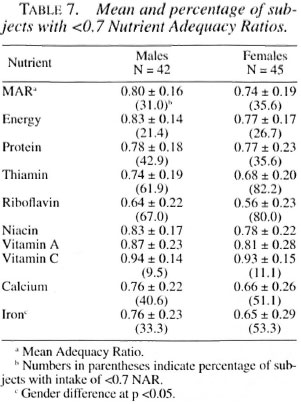
Mean Adequacy Ratios (MARs) were 0.80 and 0.74 for males and females, respectively. Nutrient Adequacy Ratios (NARs) were low for thiamin, riboflavin, calcium, and iron. In particular, more than 50% of the subjects were evaluated as having a NAR of less than 0.7 for thiamin and riboflavin. More than 50% of the females had less than 0.7 of NAR for calcium and iron.
An analysis of the nutrient intake showed a lack of food from animal sources in the diet of our subjects. Since food consumption from animal sources is thought to be related to economic conditions, we examined nutrient intake in terms of the socioeconomic status assessed by village type. There were no statistically significant differences of nutrient intake between highand low-income villagers when gender and age were controlled for.
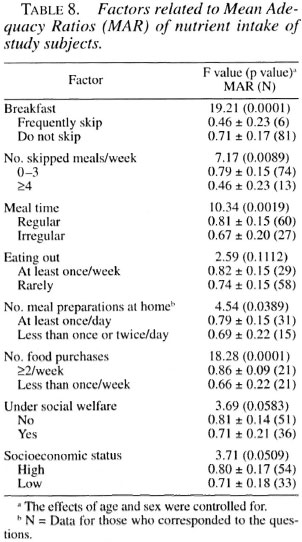
Food habits related to dietary quality. Food habits differentiated the dietary quality, MAR, for the subjects (Table 8). Those subjects who did not skip meals, ate regularly, prepared their own meals, and purchased food more frequently had better nutrient intake than did their counterparts. Social welfare status and socioeconomic status also marginally discriminated the quality of the diet.
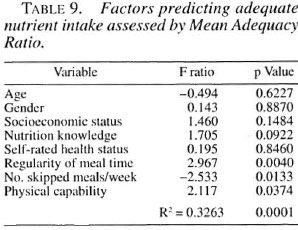
Factors predicting dietary quality. The adequacy of nutrient intake was evaluated in terms of biological (age, gender, and selfrated health status) and socioeconomic status characteristics as well as food habits (regularity of meal time and the number of skipped meals), nutrition knowledge and physical fitness. The physical fitness score was a mean of scores on the items such as performance of household work, ascending stairs and standing duration. Dietary quality measured by MAR was best predicted by food habits and physical fitness followed by nutrition knowledge as presented in Table 9.
DISCUSSION
This study was intended to assess the nutritional status of those with a history of Hansen's disease in Korea. The findings of this study indicate that the residents of resettlement villages were a nutritionally atrisk group. Their food intake was poor and their physical strength was marginal. The residents in the resettlement villages had monotonous diets largely dependent upon rice and kimchi.
When the nutrient intake was compared with the Korean RDAs, both energy-generating nutrients (macronutrients) and micronutrients were quite below the recommended amounts. Many micronutrients showed a lower percentage of the RDA values than did the macronutrients. The percent of subjects with insufficient nutrient intake (i.e., protein, thiamin and riboflavin) was more than three times higher in our study compared to the results for the general population in Korea (Ministry of Health and Social Affairs. National nutrition survey report, 1994). A similar qualitative problem of dietary intake among leprosy patients was reported in India (4). The energy intake of the Indian patients was relatively adequate, but their micronutrient intake was far from desirable. There is no reason to assume that the physiological importance of percentage units are equivalent across nutrients. Nevertheless, the association of micronutrients with the etio-pathogenesis of leprosy draws our attention to the qualitative aspect of these individuals' diets.
We also compared our findings with the data on nutrient intake of other aged people in Korea (6,9) and Ju, D.L. Assessment of dietary intake in adults living in Yeonchon area: assessment by 24-hour recall method. Master's thesis, Seoul National University, 1996). There is a large difference of nutrient intake of aged Koreans in terms of socioeconomic status. Energy intake of those from the middle class were close to the RDA while some micronutrient intake (i.e., calcium and riboflavin) was insufficient. On the other hand, nutrient intake of the older poor adults (i.e., those from the low-income families and public nursing homes) was comparable to the results of our study, which were insufficient not only quantitatively but also qualitatively. Due to a good profit from small-scale industry, the income level of the residents from the resettlement villages appears to be higher than the elderly poor in Korea, who usually had little income of their own. These findings suggest that the economic situation was not the most limiting factor which determined the quality of diet for our subjects. Rather, people who had better nutrient intake were those who ate meals regularly, skipped meals less frequently, were more physically capable and nutritionally conscious. The association of dietary quality with food habits and nutritional awareness, not with the economic situation, calls attention to a need for nutrition education since it deals with behavior and information.
In this study, as in all nonintervention studies, a problem for the interpretation of the results is the matter of causality versus association (1). Thus, the findings of this study do not permit us to make cause and effect relationships between the quality of diet and food habits, physical fitness and nutrition knowledge. These findings suggest that our Korean population in resettlement villages would benefit from nutrition education, food assistance and direct nutrition services (a congregate meal program, home meal delivery and provision of precooked foods).
Acknowledgment. We would like to thank the people of the Kyunggi Provincial Korean Leprosy Control Association and the Department of Health in Korea for their advice, support and help. Our grateful thanks go to the people in the resettlement villages who shared their lives with us.
REFERENCES
1. Ahlbom, A. and Norrel., S. Introduction to Modern Epidemiology. Chestnut, Massachusetts: Epidemiology Resources Inc., 1990.
2. Byrd, S. R. and Gelber, R. H. Effect OF Dapsone on hemoglobin concentration in patients with leprosy. Lepr. Rev. 62(1991)171-178.
3. Duncan. M. E. Leprosy in young children - past, present and future. Int. J. Lepr. 53(1985)468-473.
4. Foster, R. L., Sanchez , A. L., Stuyvesant , W., Foster, F. N., Small . C. and Lau, B. H. S. Nutrition in leprosy. Int. J. Lepr. 56(1988)66-68.
5. Gibson, R. S. Principles of Nutritional Assessment, New York: Oxford University Press, 1990.
6. Kang, M. H. Nutritional status of Korean elderly people. Korean J. Nutr. 27(1994)616-635.
7. Lew , J. A Korean Model for the Healing of Leprosy. Seoul: Lew Institute for Biomedical Research, 1993.
8. Oh, S.-Y. A nutritional perspective on children and the elderly in social welfare organization. Korean J. Nutr. 27(1994)403-409.
9. Park , H. R. Current nutritional status by different age groups. Korean J. Community Nutr. 1(1996)301-322.
10. Pedhazar, E. J. and Schmelkin, L. P. Measurement, Design, and Analysis. Hillsdale, New Jersey: Lawrence Erlbaum Associates, 1991.
11. Rhee, G. O. Development of welfare policies on aging. Korean J. Nutr. 27(1994)387-402.
12. Song , Y. S. The effect of nutrition course on the nutrition knowledge and food habits in college students. Korean J. Nutr. 19(1986)430-436.
13. Willett, W. Nutritional Epidemiology. New York: Oxford University Press, 1990.
14. Ziegler, E. E. and Filer, L. J. Present Knowledge in Nutrition. 7th edn. Washington, D.C.: International Life Science Institute Press, 1996.
1. Ph.D., Department of Food and Nutrition, Seoul National University. Seoul. Korea.
2. Sc.D., Department of Food and Nutrition, Kyung Hee University, Seoul, Korea.
3. M.S., Department of Food and Nutrition, Kyung Hee University, Seoul, Korea.
Reprint requests to Dr. Se-Young Oh. Department of Food and Nutrition, Kyung Hee University, 1 Hockidong, Dongdaemoon-gu, Seoul, Korea 130-701. Fax: 82-383-0720; e-mail: seyoung@nms.kyunghee.ac.kr.
Received for publication on 22 May 1997.
Accepted for publication in revised form on 13 January 1998.