- Volume 66 , Number 1
- Page: 59
Abnormal capillary proliferation in the iris of a leprosy patient
To the Editor:
A 63-year-old, male lepromatous leprosy patient presented with decreased vision in both eyes. He had received dapsone monotherapy for 20 years. He was clinically inactive and his skin smears were negative for acid-fast bacilli (AFB).
In 1994 the patient's right eye was operated on for cataract. At that time the right eye had a visual acuity of counting fingers, a weak orbicularis oculi muscle without demonstrable lagophthalmos, iris atrophy, a miotic pupil with posterior synechia and an intraocular pressure of 17 mmHg. During cataract extraction there was posterior capsular rupture and vitreous loss. Postoperative recovery was prolonged due to persistent uveitis requiring extended treatment with topical steroids, mydriatics and increased doses of clofazimine.
In November 1996 his right eye vision was still only counting fingers and his left eye vision had deteriorated to only perception of light. There was no acute inflammation in either eye. The left eye had had iridocyclitis in October 1994 which was treated with topical steroids and mydriatics and took a long time to resolve. There was weakness of the orbicularis oculi muscle without obvious lagophthalmos. Iris atrophy and posterior synechia were present. Since there was no acute inflammation in the left eye and no useful vision in the right eye, cataract extraction was done on the left eye. An extracapsular extraction was planned but was converted into an intracapsular extraction due to ruptured zonules. A large sector iridectomy was done and sent for histopathological examination. The vitreous face was left intact. At the close of surgery there was a large intraoperative hyphema which occupied 50% of the anterior chamber even after 5 days postoperatively. The aqueous above it developed a xanthochromic appearance. A month later the hyphema had resolved but iridocyclitis flared up in the right eye and had to be treated with topical steroids and mydriatics. An examination of the left eye done in April 1997 showed a fibrinous layer and adhesions covering the area of the sector iridectomy. The visual acuity was hand movements. The iris looked atrophic but had no rubiosis or abnormal vasculature.
The iris specimen sent for histopathological examination showed focal and diffuse infiltration of the stroma with lymphocytes, plasma cells and pigmented macrophages. The constrictor pupillae muscle was infiltrated with inflammatory cells, and there was muscle destruction. There was also an unusual proliferation of thin-walled capillaries involving the entire tissue (Fig. 1). However, in areas there were a few thick-walled hyalinized blood vessels which are normally present in the iris (Fig. 2). Some of these blood vessels showed margination of neutrophils. No AFB were seen in any of the sections.
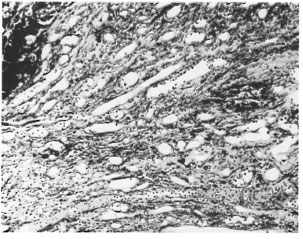
Fig . 1. Photomicrograph showing proliferating thin-walled capillaries of varying sizes hired by en-dothelium (H&E ×200).
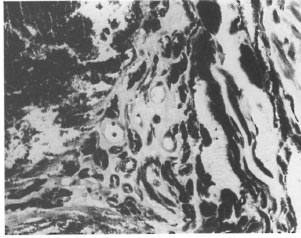
Fig . 2. Photomicrograph showing blood vessels with thick hyalinized walls characteristic of those normally found in the iris. A few scattered pigment-filled macrophages are also seen H&E ×200).
The histopathological demonstration of profuse thin-walled capillaries (Fig. 1) in the iris of this patient was inconsistent with the usual vasculature seen in the normal iris. The vessels of the normal iris appear thick walled, with the endothelial lining having a thick collar of collagen fibrils (Fig. 2).
Cavernous hemangioma occurring in the iris of a leprosy patient has been reported(2). The histopathology in this patient suggests the occurrence of a capillary hemangioma which, although by itself not significant, is an uncommon feature (1). Since the probability of a prominently vascularized tumor of the iris being a true hemangioma is low (3), and the patient had a history of having had iridocyclitis in the left eye and histology demonstrated features of chronic inflammation with lymphocytes and plasma cells infiltrating the constrictor pupillae muscle, it is possible that the abnormal vasculature could be that of a fibrovascular proliferative response to inflammation. Whatever be the etiology of the capillary proliferation, we are reporting it because of the rarity of its manifestation.
- Gigi J. Ebenezer, M.D.
Deportment of Histopathology and Experimental Pathology
Schiejfelin Leprosy Research and Training Centre
Karigiri, Vellore District
Tamil Nadu, India 632106
- Kirsteen Thompson, F.R.C.S. (Ophth.)
The Leprosy Mission
Purulia Leprosy Home and Hospittal
Purulia, West Bengal, India 723101
- Ebenezer Daniel, M.S., D.O.
Branch of Ophthalmology
Schiejfelin Leprosy Research and Training Centre
Karigiri, Vellore District
Tamil Nadu, India 632106
REFERENCES
1. Ashton , N. Primary tumours of the iris. Br. J. Ophthalmol. 48(1964)650-668.
2. Ebenezer, G. J., Daniel, E. and Job. C. K. Cavernous haemangioma of the iris in a leprosy patient. Br. J. Ophthalmol. 81(1997)610-611.
3. Ferry, A. P. Hemangioma of the iris and ciliary body. Do they exist? A search for a histologically proved case. Int. Ophthalmol. Clin. 12(1972)177-194.