- Volume 66 , Number 2
- Page: 229–31
Arsenic poisoning mimicking polyneuritic leprosy
To the Editor:
Arsenic and mercury compounds are known ingredients of Indian ethnic remedies (5). These medicines are prescribed by practitioners of Ayurvedic, Unani and other indigenous systems of Indian medicine for various cutaneous and systemic diseases. Acute arsenic exposure may produce sensory-motor neuropathy without any cutaneous changes. This could be confused for polyneuritic leprosy. We report one such case of arsenic poisoning mimicking polyneuritic leprosy.
CASE REPORT
A 65-year-old housewife presented at our neurology outpatient department with complaints of tingling, paresthesias, difficultly in rising from a squatting position and bilateral weakness of the upper limbs of 1-week duration. These symptoms developed within 3-4 days after intake of "desi-medication" from a "Hakim" for cough and expectoration. Examination showed mild anemia and generalized wasting of the extremities. The power was grade V at the wrist and ankle joints, grade III at the knee and hip joints and grade IV at the elbow and shoulder joints. In addition there was approximately 50% loss of all modalities of sensations in a "glove-and-stockitig" pattern. No other central nervous system abnormality was detected. On cutaneous examination there was generalized dryness of the extremities without any hypopigmented/hypoesthetic lesion. The classical raindrop pigmentation and palmar keratosis were absent. All of the peripheral nerves were palpable but not thickened.
A hemogram, routine urine, liver and renal function tests, and an abdominal ultrasound were within normal limits. Blood VDRL, LE cell test, Widal test and ANF were negative. A study of nerve conduction velocity revealed nonstimulability of the median, ulnar, peroneal and sural nerves due to motor-sensory axonal neuropathy. Serum arsenic level was 16.3 mcg/dl (normal <6 mcg/dl) and the urinary arsenic level was 270 mcg/liter (normal <100 mcg/liter) (1).
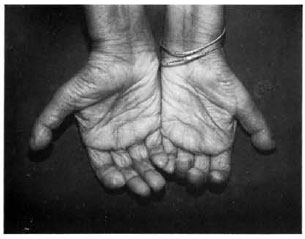
The Figure. Bilateral claw-hand deformity with concentric absorption of the fingerfips.
The patient was treated with oral penicillamine 1 gm/day. Within about 1 week there was a marked improvement in the paresthesias and muscle weakness. A repeat arsenic estimation after 7 days showed a significant decline (serum arsenic 8.3 mcg/dl, urinary arsenic 200 mcg/liter). Thereafter the dose of penicillamine was reduced to 250 mg twice daily and continued for 8 months at which time levels became normal (serum arsenic 1.7 mcg/dl, urinary arsenic 0/24 hr). The patient was referred to our dermatology department to rule out leprous neuropathy. Her slit-skin smear was negative for acid-fast bacilli (AFB) and a biopsy of the radial cutaneous nerve showed axonal demyelination with myelin loss (axonopathy) but no AFB. During follow up she gradually started to develop bilateral claw-hand deformity and concentric absorption of fingertips (The Figure). A repeat cutaneous examination after 6 months did not show any evidence of leprosy, arsenical keratosis or raindrop pigmentation.
DISCUSSION
Acute arsenic exposure results in symptoms related to the gastrointestinal tract (vomiting, bloody diarrhea, abdominal pain), the cardiovascular system (shock), and the central nervous system (cerebral edema, headache, delirium, coma and convulsions). Jaundice, renal failure, peripheral neuropathy, encephalopathy, gangrene, anemia and leukopenia, squamous cell carcinoma (5), basal cell carcinoma, Bowen's disease of the skin (6) and Mee's lines on the nails usually develop as late sequelae (3).
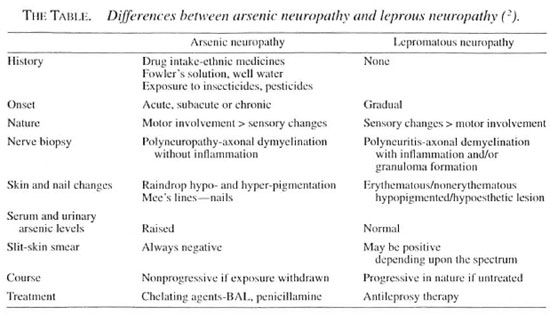
Our patient presented with acute sensory-motor neuropathy. Possibilities such as demyelinating disorders, diabetes mellitus and paraneoplastic syndromes were ruled out by various investigations. Penicil-lamine-induced neuropathy, which is due to pyridoxine (vitamin B6) antagonism, was ruled out because of the absence of associated toxicity features such as rash, fever, leukopenia, thrombocytopenia, lymph-adenopathy, proteinuria and hepatotoxicity. Moreover, it is extremely rare and occurs with high doses of penicillamine. On the basis of the patient's history of intake of indigenous medicine and raised serum and urinary levels of arsenic, the diagnosis of acute arsenic neuropathy was considered. Peripheral neuropathy develops within 10-21 days following acute or subacute arsenic exposure, but in our case symptoms appeared within 3 days. It may be due to idiosyncracy to arsenic. Weakness initially affects the lower limbs and eventually the upper limbs. In the present case both upper and lower limbs were affected simultaneously but claw-hand deformity was more striking, which has not been reported before. Even after 8 months of treatment with penicillamine when the claw-hand deformity persisted the patient was investigated for Hansen's disease. The absence of a hypo-pigmented/hypoesthetic patch, nerve thickening, negative slit-skin smear and absence of AFB in her nerve biopsy ruled out Hansen's disease. The differences between arsenic neuropathy and lepromatous neuropathy are highlighted in The Table. Thus, the claw-hand deformity could be a rare residual effect of arsenic toxicity and can be mistaken for polyneuritic leprosy in an area endemic for leprosy. We were unable to find any report of similar deformities resulting from arsenic poisoning in the reviewed literature.
The aim of the present communication is to make physicians, especially those in leprosy-endemic areas, aware of the fact that arsenic neuropathy can, on rare occasions, mimic leprosy and present with claw-hand deformity.
- Vinod Kumar Sharma, M.D., M.N.A.M.S.
Anil Soni, M.D., F.A.G.E.
S. Prabhakar, M.D., D.M.
Inderjeet Kaur, M.D., M.N.A.M.S.
Bhushan Kumar, M.D., M.N.A.M.S.
Department of Dermatology, Venereology and Leprology
and Department of Neurology
Postgraduate Institute of Medical Education and Research
Chandigarh 160 012, India
REFERENCES
1. BURTIS, C. A. and ASHWOOD, E. R. Tietz Fundamentals of Clinical Chemistry . 4th edit. St. Louis: W. B. Saunders Company, 1996.
2. DHARMENDRA. Leprosy , Volume I. Bombay: Kothari Medical Publishing House, 1978, pp. 306-309.
3. ELLENHORN, M. J. and BARCELOUX, D. G. Medical Toxicology: Diagnosis and Treatment of Human Poisoning . New York: Elsevier Science Publishers, 1988, p. 1014.
4. FELDMAN, R. G, NILES, C. A., KELLY-HAYES, M., SAX, D. S., DIXON, W. J., THOMPSON, D. J. and LANDAU, E. Peripheral neuropathy in arsenic smelter workers. Neurology 29(1979)939-944.
5. KEW, J., MORRIS, C, AIHIE, A., FYSH, R., JONES, S. and BROOKS, D. Arsenic and mercury intoxication due to Indian ethnic remedies. BMJ 306(1993)506-507.
6. SCHWARTZ, R. A. Arsenic and the skin. Int. J. Dermatol. 36(1997)241-250.
Reprint requests to Dr. Sharma at the above address or fax 91-0172-540401.