- Volume 66 , Number 3
- Page: 385–6
Lepromatous orchitis associated with seminoma
In an effort to increase the utility of the JOURNAL in continuing medical education, in this section we welcome contributions dealing with practical problems in leprosy work. Submissions to this section will undergo minimal editorial changes and may well contain controversial points. Letters to the Editor pointing out other viewpoints are welcome.
Testicular involvement in leprosy is well known. Atrophy of the testes is a fairly common condition in patients with lepromatous leprosy. Acute painful orchitis is the most common sign of testicular damage in leprosy and usually occurs during a type 2 reaction. Azoospermia and sterility have also been known to occur in patients with leprosy.1-3 We came across a borderline lepromatous leprosy patient who presented with a hard painful swelling of the scrotum that was diagnosed as a seminoma. Examination of the histopathological sections of this tumor displayed some interesting features that are reported in this paper.
CASE REPORT
A 64-year-old man presented with painful swelling of the right scrotum of 1-year duration. A year earlier he was diagnosed as having borderline lepromatous leprosy with skin smears showing an average bacterial index (BI) of 3.25+ for acid-fast bacilli (AFB). A chest X-ray showed evidence of pulmonary tuberculosis and three consecutive sputum examinations were consistently positive for AFB. An ELISA for HIV antibody was negative.
Examination of the scrotum showed a hard swelling posterior to the right testis with minimal hydrocele. A high orchidectomy was done and the excised tissue was sent for histopathological examination.
The testis showed atrophied and hyalinized seminiferous tubules with interstitial tissue infiltrated by lymphocytes and foamy macrophages which on acid-fast staining showed intracellular bacilli. The nerves coursing the testicular tissue also showed many acid-fast organisms (Fig. 1). Histologically the tumor showed the characteristic appearance of a seminoma (Fig. 2). The tumor cells infiltrated blood vessels and nerves, and tumor emboli were seen within the lymphatics. Granulomatous inflammation composed of epithelioid cells, lymphocytes and Langhans' giant cells was also seen in the tumor (Fig. 3). A diagnosis of borderline lepromatous leprosy with borderline lepromatous orchitis, pulmonary tuberculosis and seminoma was made.
DISCUSSION
Orchitis, a complication of lepromatous infection, consists of tubular atrophy and sclerosis resulting from diffuse interstitial infiltration of foamy macrophages.4 The granulomatous inflammatory infiltrate found in the tumor composed of epithelioid cells, lymphocytes and Langhan's giant cells could very well be a feature of the seminoma.5 Since Mycobacterium leprae were found in the nerve coursing through the tumor and in the granuloma, the organisms are most probably part of the borderline lepromatous disease in this patient. This case is presented because it is a rare instance of borderline lepromatous leprosy with associated lepromatous orchitis and seminoma.
- Gigi J. Ebenezer, M.D.
Head
Department of Histopathology
Schieffelin Leprosy Research and Training Center
Karigiri 632 106, Vellore District
Tamil Nadu, India
- Lionel Gnanaraj, M.S., M.Ch.
Reader
Department of Urology
Christian Medical College and Hospital
Vellore 632 004
Tamil Nadu, India
- Mannam Ebenezer, M.S.
Associate Surgeon
Department of Surgery
- Charles K. Job, M.D., F.R.C.Path., F.A.M.S.
Emeritus Scientist
Schiefklin Leprosy Research and Training Center
Karigiri 632 106, Vellore District
Tamil Nadu, India

Fig. 1. Photomicrograph showing clumps of acid-fast Mycobacterium leprae (arrows) in a nerve coursing through testicular tissue (H&E x1000).
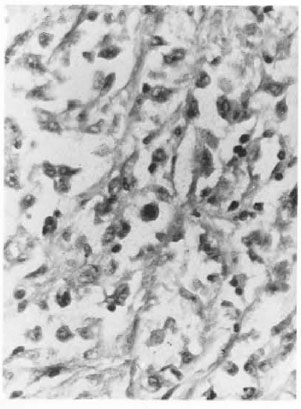
Fig. 2. Photomicrograph showing sheets of small to polyhedral cells with hyperchromatic nuclei and prominent nucleoli. Mitotic figures are also seen (H&E x200).
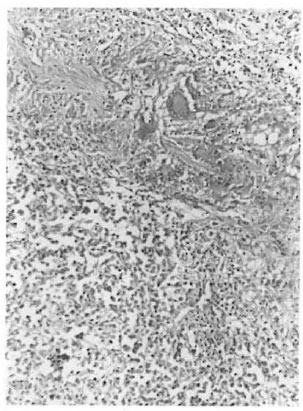
Fig. 3. Photomicrograph showing the tumor and granulomas composed of epithehoid cells, lymphocytes and Langhans' giant cells (H&E x200).
1. Job, C. K. Gynaecomastia and leprous orchitis; a preliminary study. Int. J. Lepr. 29 (1961) 423-441.
2. Kumar, B., Raina. A.. Kaur, S., Dash, R. J., Samuel, E. and Daka, B. N. Clinicopathological study of testicular involvement in leprosy. Lepr. India 54 (1982) 48-55.
3. Nigam, P., Mukhija, R. D., Kapoor, K. K., Kumar, A., Sarkari, N. B. S.. Gupta, A. K. and Mishra, S. D. Male gonads in leprosy-a clinicopathological study. Indian J. Lepr. 60 (1988) 77-83.
4. Ridley, D. S. and Job, C. K. The pathology of leprosy. In: Leprosy. 2nd edn. Hastings, R. C., ed. Edinburgh: Churchill Livingstone, 1994 p. 217.
5. Wee, Y. Q., Hang, Z. B. and Liu, K. F. In situ observation of inflammatory cell-tumor cell interaction in human seminomas (germinomas); light, electron microscopic, and immunohistochemical study. Hum. Pathol. 23 (1992) 421-428.