- Volume 71 , Number 3
- Page: 190–7
Measuring leprosy stigma - A preliminary review of the leprosy literature
ABSTRACT
A literature review was conducted to review work done to date on measuring stigma related to leprosy. References were obtained through a PubMed (Medline) search and through examining relevant bibliographies. Twelve papers were selected that addressed the issue of measurement of stigma and that contained a sample of the instrument used. Three unpublished studies were also included in the review.Studies that attempt to measure stigma can be broadly categorized in two groups, a) studies that assess the effects of stigma on the person affected, and b) surveys that assess community attitudes and/or practices. The study and questionnaire characteristics of the studies in both categories are described and compared.
The studies reviewed indicate that leprosy stigma is still a global phenomenon, occurring in both endemic and non-endemic countries. The consequences of stigma affect individuals as well as the effectiveness of leprosy control activities. Despite enormous cultural diversity, the areas of life affected are remarkably similar. They include mobility, interpersonal relationships, marriage, employment, leisure activities, and attendance at social and religious functions. This suggests that development of a standard stigma scale for leprosy may be possible. Data obtained with such an instrument would useful in situational analysis, advocacy work, monitoring and evaluation of interventions against stigma, and research to better understand stigma and its determinants.
RÉSUMÉ
Une revue de la littérature visant à revisiter le travail fait jusqu'à présent pour mesurer les stigmates associées à la lèpre, s'est appuyée sur les références obtenues par l'intermédiaire d'une recherche électronique Pubmed (Medline) et en examinant des bibliographies appropriées. Douze publications ont été sélectionnées, traitant du problème de la mesure des stigmates et qui contenait un échantillon des instruments utilisés. Trois études non publiées furent également incluses dans cette revue.Les études qui ont tenté de mesurer les stigmates peuvent être globalement divisées en deux groupes: a) les études qui évaluent les effets des stigmates sur la personne affectée et b) les enquêtes qui évaluent l'attitude et les pratiques des communautés (la stigmatisation). Le plan et les caractéristiques des questionnaires de ces enquêtes dans les deux catégories d'étude sont décrites et comparées.
La revue de ces études indique que la stigmatisation de la lèpre reste un phénomène global, sévissant à la fois dans les pays endémiques et non endémiques. Les conséquences des stigmates affectent non seulement les individus mais aussi l'efficacité des activités de contrôle de la lèpre. Malgré une diversité culturelle très importante, les aspects de la vie qui en sont affectés sont remarquablement similaires. Elles incluent la mobilité, les relations interpersonnelles, le mariage, l'emploi, les loisirs et la participation aux activités locales et religieuses. Cela suggère que l'élaboration d'une échelle standard des stigmates de la lèpre reste possible. Les données obtenues avec un tel instrument pourrait être utiles dans les analyses de situation, le travail de défense, le suivi et l'évaluation des interventions dirigées contre la stigmatisation, ainsi que la recherche pour mieux comprendre la stigmatisation et ses déterminants.
RESUMEN
Se hizo una revisión de la literatura sobre el tema del estigma en la lepra y su valoración. Como fuente de información se recurrió a PubMed (Medline), de donde se seleccionaron 12 publicaciones que hacen referencia al estigma en la lepra y al método de su medición. También se incluyeron tres trabajos que todavía no han sido publicados.Los estudios que pretenden medir el estigma de la enfermedad pueden clasificarse gruesamente en dos grupos: a) los estudios que miden los efectos del estigma en la persona afectada, y b) los estudios que miden la actitud o la reacción de la comunidad hacia los enfermos. En la presente revisión se describen y se comparan los procedimientos y los cuestionarios aplicados en las dos categorías de estudio.
Los resultados de los trabajos revisados indicaron que el estigma en la lepra es todavía un fenómeno global tanto en los países endémicos como en los no endémicos. Las consecuencias del estigma afectan tanto a los individuos como a los programas de control contra la lepra. No obstante la enorme diversidad cultural, las áreas afectadas de la vida son muy similares e incluyen desplazamiento, relaciones interpersonales, matrimonio, empleo, actividades recreativas, y asistencia a eventos sociales y religiosos. Esto sugiere que es posible desarrollar una escala de estigma estándar para la lepra. Los datos obtenidos con este instrumento podrían resultar de gran utilidad en la medición del estigma, en las investigaciones orientadas a entender mejor el estigma y sus determinantes, y en la evaluación de los resultados de las medidas tomadas contra el estigma.
Leprosy stigma is known and referred to very widely, even to the extent that the word "leprosy" (or the local term for leprosy) is used as a curse word in some countries (13). However, comparatively little systematic research has addressed the issue of stigma. Particularly, studies that have attempted to measure the level or intensity of stigma are rare. This is possibly due to the difficulty of reliably measuring psychosocial phenomena such as stigma. Currently, no standard stigma scale is widely available that could be used to measure leprosy-related stigma in different cultural settings.
METHODS
To review the work done to date on measuring stigma related to leprosy, a literature study was done. References were collected through a PubMed (Medline) search on the keywords "leprosy" combined with "stigma," "KAP," or "attitude." In addition, relevant bibliographies were studied for additional references. Only papers from the English literature that included the questions used in the study were included in the review.
RESULTS
Studies that involve some form of measurement or assessment of stigma can be broadly categorized in two groups: (i) studies that assess the effects of stigma on the person affected, and (ii) studies that assess attitudes and/or practices towards people affected by leprosy.
Studies that assess the effects of stigma on the person affected. The best developed instrument in this category is the 'Dehabilitation Scale' published by Dr. Hanna Anandaraj (1). This 52-item scale covers four areas related to stigma: family relationships, vocational conditions, social interaction, and self esteem. The items consist of positive or negative statements, with 5-point Likert-type response scales (strongly agree to strongly disagree) (25). The results are summed, divided by the maximum possible score, and multiplied by 100 to get the "score-quotient." No published studies using this scale were identified in this search.
Dr. P.K. Gopal developed a questionnaire designed to identify target groups for socioeconomic rehabilitation (Gopal, P. K. Personal communication). It contains 14 items related to attitude or practice that were to be answered with yes/no. If the respondent answered 'yes' on 50% or more of the items, (s)he was considered in need of socioeconomic rehabilitation. A large study (53,000) was conducted in India using this questionnaire, but, to my knowledge, the results have not been formally published yet (15).
The perceived participation restriction approach is being used in the development of a Participation Scale for use with people affected by leprosy or other disability. The preliminary work on that scale done in Nepal was presented during the 16th World Leprosy Congress in Brazil (Anderson, et al. Book of Abstracts. No. OSA10). The Participation Scale Development Program is an international multi-center project aiming to develop an instrument to assess, monitor, and evaluate rehabilitation needs and the impact of interventions.
Similar approaches are used in many stigma-related scales in the field of non-leprosy rehabilitation, for example the recently developed Rehabilitation Activity Profile (27), the Impact on Participation and Autonomy Questionnaire (7), scales in the field of HIV/AIDS (3) and other stigmatized infectious diseases, such as onchocerciasis (5), as well as in many other handicap scales (6).
Studies that assess attitudes and/or practices towards people affected by leprosy. Dozens of studies have been reported in which investigators have attempted to assess attitudes and/or practices towards leprosy or people affected by leprosy. Often this was in preparation for or in association with health education interventions, to see to what extent knowledge input would modify attitudes and practices among the target group(s) (9,10,11,21,28). Most studies use questionnaires or lists of statements to which respondents must reply or rate on a response scale. Reports on studies that included the scale or questionnaire used were included in the present review. The main characteristics of these studies are summarized in Table 1.
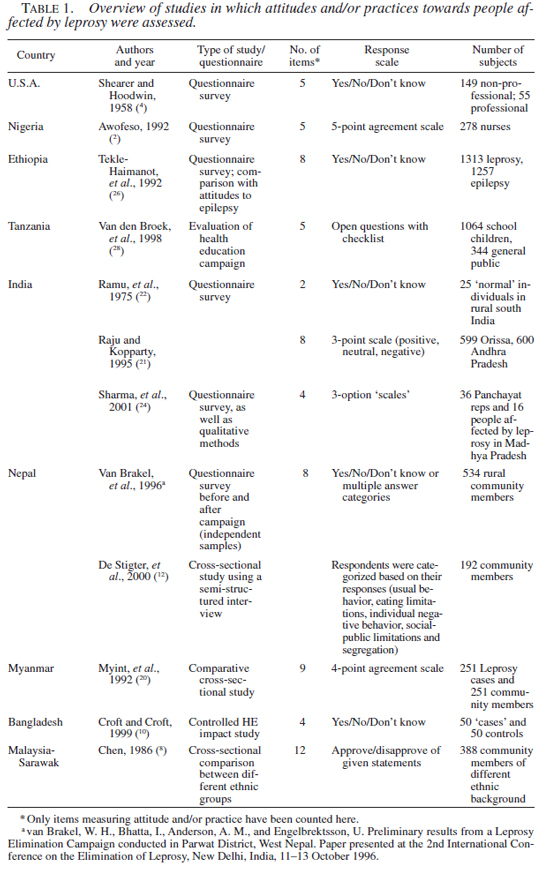
The majority of studies were cross sectional questionnaire surveys. Our own study in Nepal (van Brakel, W. H., Bhatta, I., Anderson, A. M., and Engelbrektsson, U. Preliminary results from a Leprosy Elimination Campaign conducted in Parwat District, West Nepal. Paper presented at the 2nd International Conference on the Elimination of Leprosy, New Delhi, India, 11-13 October 1996.), and the studies of van der Broek, et al. (28) and Croft and Croft (10) were health education impact assessments, comparing a community with itself in a "before and after" trial design or comparing intervention with a control community. Sometimes attitudes and practices regarding leprosy were compared between community and people affected by leprosy (20,24), or between different communities (8,21). One study compared the community attitudes towards leprosy with attitudes towards epilepsy in the same community (24).
All of the studies reviewed used questionnaires rather than scales. Most questionnaires contained items on knowledge regarding leprosy, as well as on attitude and/or practice. The number of items on attitudes and practice varied from 2 to 12. Four studies used items with "Yes/No/Don't know" response scales. Four studies used multiple category response scales (3-5 categories); one used a mixture of response options, and two used semi-structured questionnaires with open questions, one of which was a checklist of answer options.
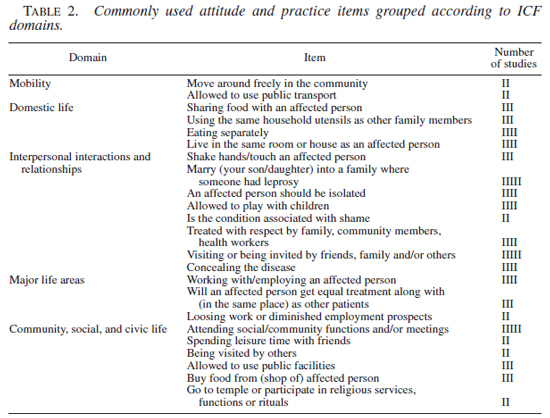
Items commonly used in the above instruments. Many areas of life may be affected by stigma. In the terminology of the new WHO International Classification of Functioning, Disability and Health (ICF), the consequences of stigma would manifest to a large extent as participation restrictions (29). The ICF recognizes nine life domains in which participation may be restricted (29). These are: (i) learning and applying knowledge, (ii) general tasks and demands, (iii) communication, (iv) mobility, (v) self care, (vi) domestic life, (vii) interpersonal interactions and relationships, (viii) major life areas, and (ix) community, social, and civic life.
In Table 2, the attitude and practice items used in two or more of the studies reviewed here have been listed, grouped according to the ICF domains. The domains covered are Mobility, Domestic life, Interpersonal interactions and relationships, Major life areas, and Community, social and civic life.
A very different approach to stigma measurement-semantic differential scales-was used in two studies described in a paper by Gussow and Tracy (16). This technique requires respondents to rate subjects such as "a person with mental illness," "a person with tuberculosis," or "a person affected by leprosy" on multi-point response scales (7-point in the quoted studies). The rating 1 represents a very unfavourable view ("bad," "sad," "worthless"), whereas 7 indicates a positive concept ("good," "happy," "valuable"). A rating of 4 is considered neutral. The ratings of the individual items are summed and the mean is calculated. In this way, one can compare community perceptions or attitudes to various conditions. Two different semantic differential scales are described in Gussow and Tracy's paper.
DISCUSSION
Stigma has been defined as "an attribute that is deeply discrediting," leading to a "spoiled identity" (14). In terms of human suffering, the consequences of stigma often outweigh the burden of physical afflictions. Many people live happily with severe physical impairments, as long as they are accepted, respected, and loved by those around them and are able to function and participate meaningfully in the society in which they live. In conditions like leprosy, HIV/AIDS, epilepsy, and mental health conditions such as schizophrenia, the stigma attached to the condition may be worse than the condition itself.
Stigma is called "enacted" when the person actually faces the effects of stigma, such as discrimination, rejection, physical abuse, loss of employment, or divorce (23). Although enacted stigma against leprosy is now less common than before, it still affects countless people worldwide. Even people related to or working with those affected may experience such stigma. "Perceived" or "felt" stigma ("self-stigma") refer to the fear of enacted stigma. Perceived stigma is a very widespread phenomenon, which may disrupt people's lives even more than enacted stigma (17,23). Perceived stigma typically occurs when a condition can be concealed [Hyland (18) cited by Heynders (17)].
Important life areas that are commonly affected by enacted stigma are people's dignity, social status, employment opportunities or job security, family relationships, and friendships. Perceived stigma may cause emotional stress and anxiety, depression, (attempted) suicide, isolation, and problems in family relationships and friendships. People have left their families, and even spouses and children, fearing the repercussions of the fact they had leprosy (19). In addition, (perceived) stigma may affect many aspects of leprosy control. People who fear the consequences of the diagnosis of leprosy may delay in presenting themselves to the health services, and thus have an increased risk of disability and continue to be a potential source of infection in the community. Fear of "being found out" and the possible consequences of that may lead to the patient discontinuing of treatment (18). Similarly, perceived stigma may lead to non-compliance with self-care routines and thus worsening of impairments.
While the presence of stigma attached to a given condition is often well recognized, the magnitude or intensity of such stigma is difficult to quantify. The question, "How strong is the stigma against leprosy in this community?" is likely to be answered with vague statements, such as "very strong," "not so strong," or "less strong than before." If stigma plays such a major role, why do we not know more about its magnitude and prevalence? The answer is that psychosocial phenomena such as stigma are difficult to measure. To date, there is no accepted scale or instrument with which stigma in the community can be quantified. Such instruments have been developed to measure stigma attached to other conditions, such as HIV/AIDS.
The studies reviewed here indicate that leprosy stigma is still a global phenomenon, occurring in both endemic and non-endemic countries. However, the questionnaires used in these studies were very different in content and structure and results are therefore difficult to compare. In addition, the items that related to attitude and practice were usually only a minority among a large number assessing leprosy-related knowledge.
Despite enormous cultural diversity, many areas of life affected by stigma are remarkably similar in different countries. They include mobility, interpersonal relationships, marriage, employment, leisure activities, and attendance at social and religious functions. These similarities suggest that it may be possible to develop a culture-free stigma scale to measure the intensity of stigma related to a condition like leprosy in a given community. The data collected with such an instrument would be very useful for a number of purposes.
(i) Understanding the situation of people affected by leprosy in a given area. This may be part of a situational analysis in preparation for a rehabilitation or health education program.
(ii) Helping in advocacy work. Data on stigma would very much strengthen the case of people involved in advocacy on behalf of those stigmatized. Such data would awaken the interest of the public to the plight of those affected by the stigma.
(iii) Monitoring and evaluation of interventions to reduce stigma in the community. Large sums of money are spent on media campaigns and other IEC interventions aiming to reduce stigma, but, to date, the impact of these is very difficult to assess.
(iv) Research. If we were able to measure stigma, we could increase our understanding of the dynamics and causes of stigma, hopefully leading to more effective interventions. We could compare stigma intensity between different people groups and communities, and try to discover factors that have helped some to overcome stigma or factors that increase the risk of stigmatization.
When assessing stigma, one should remember that stigma attached to a given condition "in the community" is not the same as the stigmatizing attitudes of individuals in that community. In other words, "community stigma" is more (or less) than the sum of stigmas held by those who make up that community [Anderson, A. (INF RELEASE Project). Personal communication.] For example, the media may portray a negative image of people with a particular condition, while many people in that community actually have a positive attitude. Similarly, services may be provided for people with the condition, but these services themselves may be stigmatizing. The classic example is that of patients with leprosy who may be able to get treatment from the general health services, but who, in many areas, are still required to attend on the "leprosy day," once a week or once a month. Attending the health facility on that particular day in itself may lead to the person being stigmatized. An assessment of stigma in a given community should therefore include an assessment of the attitudes and practices of members of that community, as well as, if possible, an "audit" of the media, legislation, and services provided. These could possibly be sub-scales of one overall stigma scale.
It should also be remembered that a stigma scale would assess reported attitudes and practices, which are not necessarily a accurate reflection of the real situation. Where possible, studies that use questionnaires or scales to assess stigma should therefore be complemented and validated by qualitative methods, such as participant observation, focus group discussions, and in-depth interviews. Another means to validate the results obtained from a community stigma survey would be to compare the results with information obtained from those affected by the stigma through an instrument such as the Participation Scale (A culture-free questionnaire-based instrument, currently being developed in an international multi-center study; for more information, please contact the author) or Anandaraj's Dehabilitation Scale (1).
CONCLUSION
Many attempts have been made to assess the intensity and qualities of stigma attached to leprosy, but no standard instrument has been developed for this purpose. The consequences of stigma are far-reaching, affecting the lives of countless individuals, as well as the effectiveness of leprosy control programs. The consequences of stigma are remarkably similar in many different cultural settings. The development of a standardized stigma scale is recommended.
REFERENCES
1. Anandaraj, H. Measurement of dehabilitation in patients of leprosy-a scale. Indian J. Lepr. 67(2)(1995)153-160.
2. Awofeso, N. Appraisal of the knowledge and attitude of Nigerian nurses toward leprosy. Lepr. Rev. 63(2)(1992)169-172.
3. Berger, B.E., Ferrans, C.E. and Lashley, F.R. Measuring stigma in people with HIV: psychometric assessment of the HIV stigma scale. Res. Nurs. Health. 24(6)(2001)518-529.
4. Booth, R.J. and Ashbridge, K.R. A fresh look at the relationship between the Psyche and Immune system: teleological coherence and harmony of purpose. J. Mind-Body Health. 9(2)(1993)8-23.
5. Brieger, W.R., Oshiname, F.O. and Ososanya, O.O. Stigma associated with onchocercal skin disease among those affected near the Ofiki and Oyan Rivers in western Nigeria. Soc. Sci. Med. 47(7)(1998)841-852.
6. Cardol, M., Brandsma, J.W., de Groot, I.J., van den Bos, G.A., de Haan, R.J. and de Jong, B.A. Handicap questionnaires: what do they assess? Disabil. Rehabil. 21(3)(1998)97-105.
7. Cardol, M., de Haan, R.J., RN, de Jong, B.A., van den Bos, G.A.M. and de Groot, I.J.M. Psychometric properties of the impact on participation and autonomy questionnaire. Arch. Phys. Med. Rehabil. 82(2001)210-215.
8. Chen, P.C. Human behavioural research applied to the leprosy control programme of Sarawak, Malaysia. Southeast Asian J. Trop. Med. Public Health. 17(3)(1986)421-426.
9. Chen, P.C. and Sim, H.C. The development of culture-specific health education packages to increase case-finding of leprosy in Sarawak. Southeast Asian J. Trop. Med. Pub. Health. 17(3)(1986)427-432.
10. Croft, R.P. and Croft, R.A. Knowledge, attitude and practice regarding leprosy and tuberculosis in Bangladesh. Lepr. Rev. 70(1)(1999)34-42.
11. Crook, N., Ramasubban, R., Samy, A. and Singh, B. An educational approach to leprosy control: an evaluation of knowledge, attitudes and practice in two poor localities in Bombay, India. Lepr. Rev. 62(4)(1991)395-401.
12. de Stigter, D.H., de Geus, L. and Heynders, M.L. Leprosy: between acceptance and segregation. Community behaviour towards persons affected by leprosy in eastern Nepal. Lepr. Rev. 71(4)(2000)492-498.
13. Frist, T. Don't Treat Me Like I Have Leprosy! 1st edn. London: TALMILEP. 1996
14. Goffman, E. Stigma: Notes on the Management of Spoiled Identity. Englewood Cliffs, New York: Prentice-Hall. 1963
15. Gopal, P.K. Social and Economic Integration. Tokyo: Sasakawa. 1998
16. Gussow, Z. and Tracy, G.S. The phenomenon of leprosy stigma in the continental United States. Lepr. Rev. 43(2)(1972)85-93.
17. Heynders, M.L. 2002. Understanding adherence in leprosy. Ph.D. thesis, South Bank University, London, U.K.
18. Hyland, J.A. 1993. A socio-cultural study of leprosy in Nepal: compliance, patient illness career patterns, and helath education. Ph.D. dissertation, University of Tasmania.
19. Kaur, H. and van Brakel, W.H. Dehabilitation of leprosy-affected people: a study on leprosy-affected beggars. Lepr. Rev. 73(2002)346-355.
20. Myint, T., Thet, A.T., Htoon, M.T. and Win, M. A comparative KAP study of leprosy patients and members of the community in Hlaing and Laung-Lon townships. Indian J. Lepr. 64(3)(1992)313-324.
21. Raju, M.S. and Kopparty, S.N. Impact of knowledge of leprosy on the attitude towards leprosy patients: a community study. Indian J. Lepr. 67(3)(1995)259-272.
22. Ramu, G., Dwivedi, M.P. and Iyer, C.G.S. Social reaction to leprosy in a rural population in Chingleput District (Tamil Nadu). Lepr. India. 47(3)(1975)156-169.
23. Scambler, G. Stigma and disease: changing paradigms. Lancet. 352(9133)(1998)1054-1055.
24. Sharma, V., Girdhani, M. and Rajput, Y. Leprosy-Perception & Practices of Bhils in Jhabua. DANLEP. Bhopal: Center for Advanced Research and Development, 2001.
25. Streiner, D.L. and Norman, G.R. Health Measurement Scales. A Practical Guide to Their Development and Use. Oxford: Oxford University Press, 1989.
26. Tekle-Haimanot, R., Forsgren, L., Gebre-Mariam, A., Abebe, M., Holmgren, G., Heijbel, J. and Ekstedt, J. Attitudes of rural people in central Ethiopia towards leprosy and a brief comparison with observations on epilepsy. Lepr. Rev. 63(2)(1992)157-168.
27. van Bennekom, C.A.M., Jelles, F. and Lankhorst, G.J. Rehabilitation Activities Profile: the ICIDH as a framework for a problem-oriented assessment method in rehabilitation medicine. Disab. Rehab. 17(1995)169-175.
28. van den Broek, J., O'Donoghue, J., Ishengoma, A., Masao, H. and Mbega, M. Evaluation of a sustained 7-year health education campaign on leprosy in Rufiji District, Tanzania. Lepr. Rev. 69(1)(1998)57-74.
29. World Health Organization. International Classification of Functioning, Disability and Health(ICF). Geneva: World Health Organiation, 2001.
M.D., M.Sc., Ph.D., TLM Research Resource Center 5 Amrita Shergill Marg, New Delhi-110003, India.
Reprint requests to: Dr. Wim H. van Brakel, Consultant for Leprosy and Tuberculosis, Royal Tropical Institute (KIT), Amsterdam, the Netherlands. E-mail: wvbrakel@mail.com
Received for publication on 15 November 2002.
Accepted for publication on 7 July 2003.