- Volume 65 , Number 2
- Page: 246–51
An anatomist in leprosyland (on a contribution f rom mid-nineteenth century India)
Editorial opinions expressed are those of the writers.
The scientific era in the understanding of the neurology of leprosy was inaugurated by Danielssen and Boeck in Norway in 1847,1 who described some of the prominent features of nerve involvement. Fifteen years later in 1862, Danielssen published a more detailed evaluation of the gross changes in the nerves, emphasizing the relationship to anesthetic cutaneous macules.2 The "granulomatous" nature of the pathology in leprosy skin and nerve was recognized, the "Lepra cell" described, and "axis cylinder and myelin" degeneration were noted by the renowned pathologist Rudolf Virchow of Berlin in his publication of 1865.3 It is not surprising that later treatises implied that this phase of leprology comprised discoveries of influential pioneers working on the European mainland.1
Overseas contributions were also to be expected at this time, however, if only because leprosy was so prominent a feature of the medical landscape of the European colonial possessions in Asia and elsewhere that the disease would certainly have attracted the attention of research-minded officers of colonial medical services.
As far as "British India" was concerned, just such a medical officer, Henry Vandyke Carter (1831-1897), was in Bombay studying the leprosy patients at the Jamsetjee Jeejeebhoy Hospital soon after his arrival in India in 1859, having already earned some fame in England as dissector and artist in the first edition of Gray's Anatomy (Fig. 1) Carter's 30 years of activity in India have been described earlier.4
Fig. 1. Title Page of the first edition of Gray's Anatomy 1858 (From the reprinted edition by Magpie Books, London, 1993).
The present account calls attention to Carter's early nerve studies in little-known but meritorious publications (in 1862 and 1863)5-6 on "this terrible scourge of the in digenous population of India, [which] though widely prevalent and pitiably destructive in its effects, has attracted but slight attention on the part either of the ruling powers or our own profession... "
"The Pathology of Leprosy in India," he wrote "is a subject of enquiry well deserving investigation. This disease is doubtless associated with well-known hygienic conditions; but it has also a special diathesis... it is probably the only disease known which is confined (if we may except the renal organs) to the nerves and the sentient skin."
In September I860,5 as Professor of Anatomy at the Grant Medical College, he laid before the Medical and Physical Society of Bombay a dissected leprous upper limb, marking the diseased nerves as "the lower part of the radial, the median above the wrist, and the ulnar at the elbow." Later, in December 1861, the minute morbid anatomy of the nerves was described, he believed, "for the first time, as the only other observers (Messrs. Danielssen and Boeck in Norway) who have given any details concerning this subject, do not seem to have made use of the microscope."
By 1862, he was convinced that "the anaesthesia-the characteristic feature of all varieties of leprosy-is owing to a diseased condition which is confined to the nerves supplying the benumbed parts. The nerve centres [Note: the central nervous system] are not necessarily affected... "
In his first monograph on leprosy,6 he classified the "eruption" and the neuropathy as seen in 200 cases, and appended findings in "16 mortisections... [which] include dissection of the nerves of one side of the body (Fig. 2a) and subsequent microscopic examination of the diseased structures... It is here that interest chiefly centres... In order to render them intelligible, the normal structure, as well as the anatomical distribution of the nerves should be recalled to mind, and the more clearly they are recollected, the better will the connection between the symptoms of leprosy and the morbid alterations which accompany it, be understood."
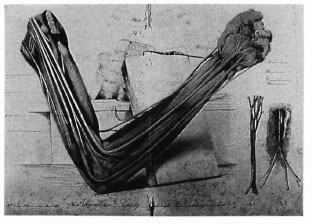
Fig. 2a. Carter's illustration of his nerve dissection. Note the representations of the "intra-neural plexuses" and of the relationship of cutaneous nerve enlargement to the deep fascia. This dissection/illustration is Plate IX From his book of 1874,4 but was executed by him in 1862.
"... A healthy nerve is uniform in diameter, of an opaque whitish or yellow colour, and rather lustrous hue... When of moderate size it will be found to consist of several funiculi (cords or strands), readily visible through its coat, which not only run parallel to each other but frequently communicate, so that numerous plexuses are formed within the nerve trunk itself; these are particularly evident in the larger nerves, and their significance has been rather overlooked, I think, by anatomists; such an interchange of nerve tubules is hereby effected that it becomes impossible to trace far those of an individual funiculus, hence disease of the latter may lead to symptoms anywhere in the area supplied by the whole nerve. Each funiculus is provided with a sheath (neurilemma) [the perineurium] and is itself composed of clusters of nerve tubules similarly isolated; one or more of these alone may be diseased in leprosy. The nerve tubules are classed as large (motor?) and small (sensory?) according to their size, and there is no question that the latter may be affected to the exclusion of the former, so that the disease of even a compound nerve may cause anaesthesia alone... "
"... The diseased nerve is swollen, but not abruptly so, and of a dull reddish grey or semi-translucent aspect; rounded and firm. Its coat of connective tissue is little changed, the funiculi alone being the seat of disease. These, enlarged and grey in colour, impart a streaked or marbled appearance, and when the nerve is cut across they start up, separate and firm, almost as if previously under some degree of tension; in the healthy nerve they rather droop. On further examination, the clusters of nerve-tubules are found to have mostly disappeared, their place being taken by a clear gelatine-like deposit, which has separated and compressed them; this is provided with nuclei and fibres, the latter curiously arranged round each tubule, and thus 'mapping out', as it were, the area into rounded or polygonal spaces, in each of which lie the remains of one or two altered nerve tubules... (Fig. 2b).
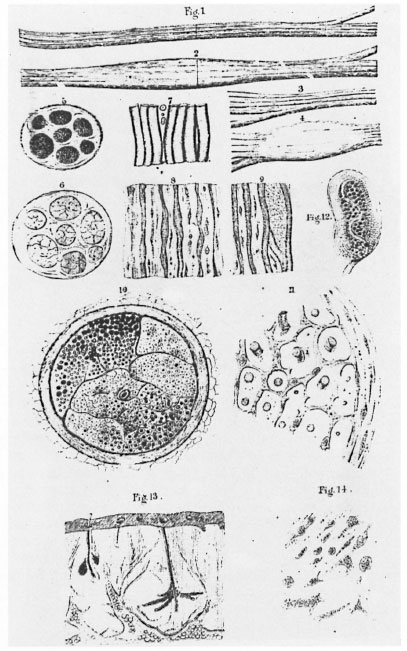
Fig. 2b. Details of the gross and microscopic features of leprous contrasted with normal nerve.
"... Thus it will be seen that enlargement and diminished opacity are the fundamental changes which nerves exhibit... the amount of enlargement varies From just above the normal size (at the seat of disease, above or below it, the nerve may be smaller than natural) to more than twice that: the colour may be grey, reddish-grey... or very rarely a dead opaque white: the consistence of all degrees From almost flabby to semi-cartilaginous, but generally firmer than natural... The cutaneous nerves are altered in a similar manner.
"... These changes do not occur indiscriminately in the course of the nerves, but make their appearance at certain selected spots; for the compound trunks where they are most superficially placed, for the cutaneous nerves immediately after they have perforated the deep fascia (Fig. 3). As regards the former, the nerve trunk above the iocus morbi' may be unchanged, below it is usually atrophied, but occasionally almost normal in appearance and structure: the apparent extent of disease may be limited to two or three inches, but it is often considerably more; in both sets of nerves the terminal branches will be found atrophied and pearly in aspect, being, in wellmarked cases, evidently incapable of performing their functions... "
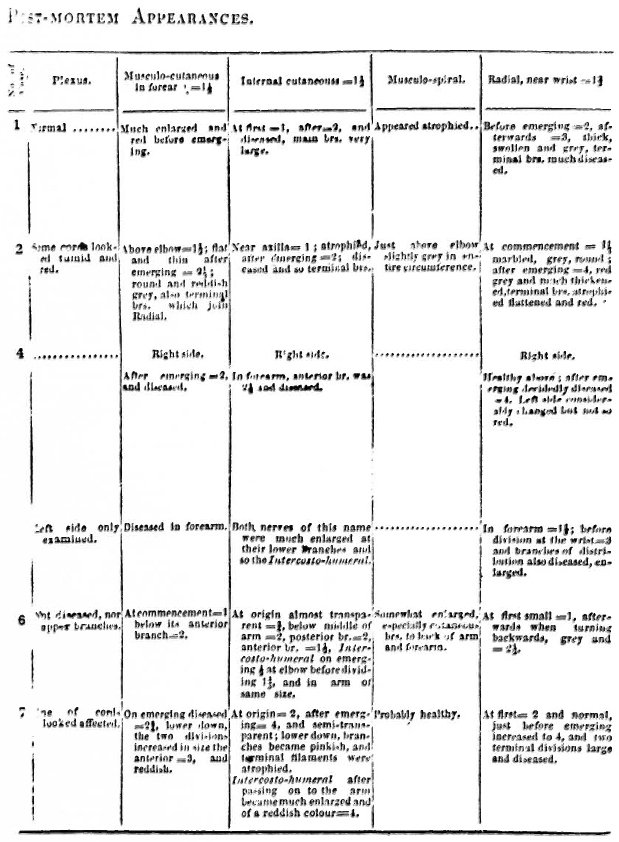
Fig. 3. Part of Carter's Tabulation of Morphological Changes in the Cutaneous Nerves in Leprosy PostMortem.
"A very interesting fact connected with the nerves of compound function is recorded... viz., that the sensory or cutaneous segment alone may be diseased being traceable by the eye for some distance upwards in continuation of the altered cutaneous branch, after it has joined the main trunk: this fact, as well as others, also show that the morbid changes proceed From the periphery towards the centre, as might have been anticipated... "
"... There is little to be said on the comparative liability of any nerve to disease, as in cases at all advanced (and such only have as yet been investigated) almost the whole of the nerves named in the above list were found implicated; it may be inferred however, that the Ulnar and Radial nerves in the upper, and the musculo-cutaneous in the lower extremities, are oftenest affected; they supply the dorsum and inner side of the hand, and the dorsum of the foot: and least often the branches of the fifth cranial nerve on the face..."
"These [histologic] observations unequivocally demonstrate the... morbid process in the nerves themselves, so that some of their components may continue to perform their functions, while others certainly could not... on the other hand a nerve may appear healthy enough, and yet a segment of it be decidedly ineffective. Histologists have not sufficiently determined the characters of motor, sensory and sympathetic nerve tubules to enable pathological enquirers to settle a question like the present, but it would appear From the symptoms and the special tendencies of leprous disease, that the last-named elements of a compound nerve are those peculiarly affected... "
"... I assume that disease begins not at the periphery of the nerves, but at certain elective points, below which, and sometimes above, they become atrophied... as regards the cutaneous nerves that it may be otherwise, as the wasting below the seat of lesion is not always that of mere atrophy, but rather a conversion into tough fibrous tissue with no diminution of size, which would indicate previous effusion or deposit between the tubules... "
"... With regard to the nature of the disease, on first impression it would appear to be inflammatory, for the primary symptoms include local pain and tenderness of the nerves... My own opinion is that the change [in the nerves] is one of fibrous conversion or degeneration, commencing... in the envelope or limiting membrane of the nerve tubules (which is possible), or immediately on its exterior, with the effusion of an organizable material... Evidently there is no real hypertrophy of the nerves."
"... Such are the results of my enquiries into the structural pathology of leprosy: but I am fully aware of many deficiencies in these observations... which call for the attention of those favourably placed... to furnish, so that this widespread and fearful malady shall no longer remain an ignored subject."
COMMENT
The conspicuous naked-eye changes in the peripheral nervous system in leprosy lend themselves admirably to display but the anatomist in Carter also was able to make some additional observations, viz., that nerve enlargement, firmness and loss of lustre, "... do not occur indiscriminately in the course of the nerves, but make their appearance at certain selected spots; for the compound trunks where they are most superficially placed, for the cutaneous nerves immediately after they have perforated the deep fascia."
He apparently had an inkling of the direction of spread of the disease process in the nerves... "very interesting fact... viz., that the sensory or cutaneous segment alone may be diseased being traceable by the eye for some distance upwards in continuation of the altered cutaneous branch, after it has joined the main trunk: this fact, as well as others, also show that the morbid changes proceed From the periphery towards the centre, as might have been anticipated."
The 1863 monograph also documents, probably for the first time, the significance of the "rather overlooked" feature of the intraneural plexuses formed by funiculi. Over a hundred years later Sunderland's7 more sophisticated studies emphasized this very intra-neural feature in the centripetal dissemination of leprosy bacilli and inflammation From cutaneous to mixed cutaneousmotor funiculi.
Virchow in 1865 cited, somewhat patronizingly, Carter's microscopic nerve studies, implying that they only confirmed what he (Virchow) and Danielssen had already found. "The recent observations of Carter agree so completely with those of Danielssen and myself in main points that there can be no doubt of the validity of the evidence."3 It is unfortunate that Carter's major insights into the neuro-anatomy of leprosy also seem to have been unappreciated.
Acknowledgment. The assistance of medical students A. Schultz and S. Bleuel in translating the relevant passage From Klingmuller' is greatly appreciated.
- Shubhada S. Pandya, M.B.B.S.
Research Officer
Acworth Leprosy Hospital Society for Rehabilitation and Education in Leprosy
Bombay 400 031, India
1. Klingmuller, V. Die Lepra. Berlin: Verlag von Julius Springer, 1930, pp. 452-453.
2. Lie, H. P. The classification of leprosy. Int. J. Lepr. 4(1936) 35-44.
3. Virchow, R. Die Krankhaften Geschwulste. Berlin, 1865. Translated by G. L. Fite. Int. J. Lepr. 22 (1954) 205-217.
4. Pandya,S. S. Henry Vandyke Carter (1831-1897); Medical Artist and Scientist. Lepr. India 43 (1971) 19-23.
5. Carter, H. V. Case of anaesthetic leprosy, with post-mortem examination and remarks. Trans. Med. Phys. Soc. Bombay New Series 7 (1862) Appendix xxviii-xxix.
6. Carter, H. V. On the symptoms and morbid anatomy of leprosy; with remarks. Trans. Med. Phys. Soc. Bombay New Series 8 (1863) 1-104.
7. Sunderland, S. The internal anatomy of the nerve trunks in relation to leprosy. Brain 96 (1973) 865-888.