- Volume 65 , Number 3
- Page: 374–5
Histoid nodules of leprosy on the lip
To the Editor:
A 45-year-old man was seen in June 1990 for multiple asymptomatic nodules on the upper lip and nose of 3 months' duration. He gave a history that in 1981 he had multiple skin patches which were diagnosed as lepromatous leprosy by a local leprologist and was treated with dapsone 50 mg daily. He discontinued the treatment after 2 years without consulting the doctor. The patches had disappeared at that time. The nodules on the lip and nose developed gradually since January 1990. There was no fever or other constitutional symptoms.
Examination revealed multiple, well-circumscribed, firm, dome-shaped, smooth, nontender nodules on the upper lip and nose skin (The Figure). The nodules on the nose were skin-colored while those on the lip were coppery-red. The nodules appeared as if arising from normal-looking skin and mucosa. The nodules at the alar nasi coalesced to form a cluster of nodules. There were no other skin or mucosal lesions elsewhere on the body, although there was wrinkling of the skin of the pinna of the ears.
Routine laboratory tests on blood (total and differential leukocyte count, ESR, hemoglobin), urinalysis and renal and liver function tests were within normal limits. A blood VDRL (Venereal Disease Research Laboratory) test was negative. An X-ray of the chest was normal. Slit-skin smears from the earlobes, forehead, chin and dorsa of middle fingers did not show acid-fast bacilli (AFB), but those taken from nodules of the nose and lip revealed numerous AFB, the morphologic index (MI) being 80% and bacterial index (BI) 5+. There were no AFB in the slit-skin smears taken from normalappearing skin of the nose and mucosa of the lip. A histopathological study of the biopsies of the nodules on the nose and lip revealed circumscribed collections of thin, spindle-shaped histiocytes arranged in a whorl pattern throughout the dermis. A few lymphocytes also were seen. Ziehl-Neelson-stained tissue sections showed numerous, long, uniformly stained AFB arranged in parallel bundles inside the histiocytes. There were no globi.
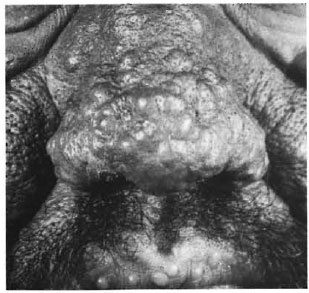
The Figure. Histoid leprosy nodules on the nose and upper lip.
The patient was treated with multidrug therapy consisting of dapsone, rifampin and clofazimine as recommended by WHO (WHO/MDT) for multibacillary cases (5). There was a gradual fall in the MI, and it became zero at the end of 6 months of MDT The nodules regressed slowly and when seen after 3 years of MDT, they all had disappeared leaving faint atrophic macules. The MI remained zero and the BI had fallen to 2+, after which he was lost for follow up.
Histoid leprosy originally described by Wade (3) is a variant of lepromatous leprosy. It is characterized by the development of firm, hemispheric, dome-shaped, welldefined nodules on an apparently normallooking skin. Many cases occur during a relapse after dapsone monotherapy or may arise per se without any prior chemotherapy. The nodules tend to arise in unusual body sites, such as the lower back, loins or axillae or over the chest and neck (1).
Clinical and histopathological features of the nodules in our patient suggested a diagnosis of histoid leprosy. The lesions appeared as a relapse of lepromatous leprosy, probably due to inadequate dosage and duration of dapsone monotherapy. The possibility of infection with dapsone-resistant Mycobacterium leprae also exists in our case, although we could not prove it due to the lack of facilities for animal inoculation studies. WHO/MDT resulted in complete clinical cure of leprosy in this patient, although a few dead bacilli persisted at the site of the nodules.
Another interesting feature observed here was the presence of histoid nodules on the lip mucosa. Unlike the nose lesions which were skin-colored and appeared in clusters, the lip lesions were discrete and copperyred. This color variation is probably due to the increased vascularity and decreased melanization of the lip mucosa. Involvement of the mucous membrane is quite unusual in histoid leprosy, although rarely nodules have been reported to develop on the mucosal surface of the hard palate and glans penis (2), and may also occur in the nasal mucosa (4).
REFERENCES
1. PFALTZGRAFF, R. E. and RAMU. G. Clinical leprosy. In: Leprosy. 2nd cdn. Hastings, R. C. cd. Edinburgh: Churchill Livingstone, 1994, pp. 237-287.
2. RAMANUJAM, K. and RAMU, G. Wade's histoid lepromatous leprosy: report of a clinical study. Lepr. India 41(1969)293-297.
3. WADE, H. W. The histoid variety of lepromatous leprosy. Int. J. Lepr. 31(1969)129-142.
4. WADE. H. W. and TOLENTINO, J. C. The histoid variety of lepromatous leprosy. (Abstract) Int. J. Lepr. 31(1963)608-609.
5. WHO STUDY GROUP. Chemotherapy of leprosy for control programmes. Geneva: World Health Organization, 1982. Tech. Rep. Sen 675.
M.B.B.S., M.D., D.V.D., M.N.A.M.S. Professor of Dermato-Venereology, Medical College Hospital, Calicut 673 008, Kerala, India.