- Volume 65 , Number 4
- Page: 495–7
A multicenter study of recombinant lnterferon-alpha2b in the treatment of multibacillary leprosy
This department is for the publication of informal communications that are of interest because they are informative and stimulating, and for the discussion of controversial matters. The mandate of this JOURNAL is to disseminate information relating to leprosy in particular and also other mycobacterial diseases. Dissident comment or interpretation on published research is of course valid, but personality attacks on individuals would seem unnecessary. Political comments, valid or not, also are unwelcome. They might result in interference with the distribution of the JOURNAL and thus interfere with its prime purpose.
To the Editor:
Lepromatous leprosy has well-documented deficiencies in the macrophage regulation system (9). The role of cytokines, such as gamma-interferon (IFN-γ), interleukin 2, tumor necrosis factor in macrophage stimulation (8), natural killer (NK) cell activity and antibody-dependent cellmediated cytotoxicity (ADCC) (3), have been described. Combination chemotherapy utilizing drugs like dapsone, rifampin, and clofazimine (6) and newer groups of drugs such as macrolides (7) and quinolones (11) have been shown to be effective. The rate of fall of the bacterial index (BI) is about 1 log per year. The search is now on to try to achieve a higher cell kill and to clear the dead bacilli faster.
The treatment of patients having lepromatous leprosy with local IFN-yhas been tried before (2,5,12). They are shown to have rapid bacillary clearance and increased H2O2, release by macrophages when IFN-γ was Injected locally (13). IFN-yhas a poor muscle and skin absorption along with a short half-life of 25-30 min (4).
Alpha-interferon (IFN-α) has been used extensively to treat malignancies (1) and viral infections (10). The role of IFN-a on NK cell activity and ADCC has been documented in vitro (3). The clinical efficacy of IFN-a in leprosy has not been evaluated before.
MATERIALS AND METHODS
Forty patients with lepromatous leprosy were randomized to the multidrug therapy (MDT) arm or MDT-interferon (MDTI) arm of our study. The treatment on the MDT arm consisted of dapsone 100 mg and clofazimine 50 mg daily along with rifampin 600 mg and clofazimine 300 mg monthly, the duration of treatment being 24 months. The MDTI arm consisted of the above treatment along with alpha-interferon 2b (IFN-a2b) at a dose of 3 million units subcutaneously twice a week for 6 weeks. The clinical features, BI, histology and lepromin reactivity were documented at baseline and at 3 months. The clinical features will be followed up monthly for 24 months and yearly thereafter. While the BI was read as it normally is, the histology was scored according to a predetermined histological scoring system.
Statistical methods. The Mann-Whitney U test for unpaired ordinal variables and an unpaired / test for continuous variables were used.
RESULTS
We were able to evaluate the histology for 30 patients (20 on the MDTI arm and 10 on the MDT arm). There were 37 patients for whom we were able to evaluate the BI (19 on the MDTI arm and 18 on the MDT arm). The baseline median histopathological score was 3 for both the MDTI and the MDT arms. The mean Bis also were similar, 3 and 3.1 for the MDTI and MDT arms, respectively. The mean fall in the BI was 1.526 and 0.547 for the MDTI and MDT arms, respectively, the difference of 0.98 (95%CI 0.45-1.50) being significant (p = 0.001) (The Table, The Figure). The mean fall in the histopathology score was 0.85 and 0.2 in the MDTI and MDT arms, respectively, this too being significant (p = 0.029).
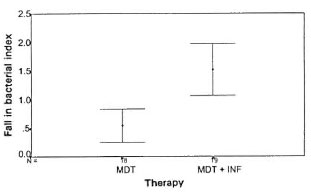
The Figure. Fall in bacterial index in the MDTand MDTI arms was 0.547 and 1.526, respectively, thedifference of 0.98 (95%Cl 0.45-1.50) being significant (p = 0.001).
Lepromin reactivity was negative in all patients at baseline and continued to be so after 3 months.
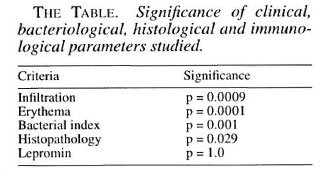
Clinical features studied included infiltration and erythema, the differences in preand post-treatment scores were significant, p = 0.0009 and p = 0.0001, respectively.
There was one type 1 reaction on the MDT arm and one type 2 reaction on the MDTI arm. Apart from malaise and mild fever following the injections there was no major side effect attributable to IFN-α.
DISCUSSION
The bacterial cell kill after chemotherapy is probably effective, but dead bacilli remaining in the soft tissue often contribute to disease morbidity. The fall in the BI is one of the modes of following up the load of dead bacteria. Cytokines play a role in the activation of macrophages which is important in the removal of bacteria and cells from the dermis. The addition of a short course of IFN-or to the MDT seems to have significantly enhanced the fall in the BI at an early stage of the treatment itself.
The baseline histology in all of the patients revealed a clear subepidermal layer and foam cells. The patients who were given IFN-a along with the MDT had a more rapid clearance of foam cells which could, again, signify an enhanced cell-mediated clearing of the dead cells.
Lepromin testing is a measure of the cellmediated activity manifested by the body; this did not seem to be altered by the addition of IFN-a to the MDT during the period of the study.
While these are preliminary observations, IFN-α does seem to favorably influence the BI and the histology when added to MDT in patients with lepromatous leprosy. The long-term follow up of these patients will reveal a more definite picture of the alterations of the natural history of the disease, the observations of which will be a part of future communication.
- Dr. R. Ganapati
Dr. V. V. Pai
Dr. Udai Banerji
Bombay Leprosy Project
Vidnyan Bhavan
11 V.N. Purav Marg
Sion Chunnabhatti Road
Bombay 400 001, India
- Dr. Jaykar Thomas
Institute for Child Health and Hospital for Children
Chennai, India
- Dr. B. Saha
School of Tropical Medicine
Calcutta, India
REFERENCES
1. ALLEN, N. C, RICHARD, S. M. and SHEPARD, P. C. A. U.K. Medical Research Council randomized multicenter trial of interferon alpha for chronic myeloid leukemia, improved survival irrespective of cytogenetic response. Lancet 345 (1995) 1392-1397.
2. BHUTANI, L. K., MLHRA, N. K., NUNDY, S. and NATH, I. Leprosy. Lancet 345 (1995) 697-703.
3. CHIPLUNKAR, S. V., DHSHMUKH, M. V., SAMSON, P. D., BUTI.IN, C. R., BHATKI, W. S., CHUI.I.AWALA, R. G., DEO, M. G. and GANOAL, S. G. Natural killercell-mediated and antibody-dependent cellular cytotoxicity in leprosy. Int. J. Lepr. 58 (1990) 334_341.
4. ClRELLI, R. and TYRING, S. K. Major therapeuticuses of interferons. Clin. Inimunother. 3 (1995) 27-87.
5. DAMASCO, M. H. S., SAKNO, E. N., LOBAO, A. S., AI.VARLNOA, F. B. F, PORTO, J. A., ROSANKAIMHR, F. and KAPLAN, G. Effect of cutaneous cell-mediated immune response to rIFN-gamma on Mycobacterium leprae viability in the lesions of lepromatous leprosy. Braz. J. Med. Biol. Res. 35 (1992)457-465.
6. GANAPATI, R., PAI, R., GANDEWAR, K. L. and THRESSIA, X. J. For how long should a multibacillary leprosy patient be treated? Indian J. Lepr. 61 (1989)467-471.
7. Ji, B., JAMET, P., PERANI, E. G., Sow, S., LlEN-HARDT, C, PITINON, C. and GROSSKT, J.-H. Bactericidal activities of a single dose of clarithromycin plus minocycline, with or without ofloxacin, against Mycobacterium leprae in patients. Antimicrob. Agents Chemother. 40 (1996) 2137-2141.
8. KAPLAN, G Recent advances in cytokine therapy in leprosy. J. Infect. Dis. 167 Suppl. 1 (1993) 18-22.
9. MAKONKAWKKYOON, S., KASINRLK, W., SAPAJATURA, V., HlRUNPETCHARAT, C. and VlTHARASAI, V. Immunological defects in leprosy patients; intcrleukin 1, interleukin 2, and interferon production in leprosy patients. Int. J. Lepr. 58 (1990) 311-318.
10. MAURACHER, E. H. Low dose interferon alpha 2b for chronic hepatitis B in Asian countries. Gut 34 Suppl. 2(1993)99-100.
11. MOCHIZUKI, Y., OlSHI, M., NlSHlYAMA, C. and IIDA, T. Active leprosy treated effectively with ofloxacin. Intern. Med. (Tokyo) 35 (1996) 749-751.
12. SAMPAIO, E. P., MALTA, A. M., SARNO, E. N. and KAPLAN, G. Effect of rhuINF-y treatment in multibacillary leprosy patients. Int. J. Lepr. 64 (1996) 268-273.
13. SHIVA SAI, K. S. R., PRASAD, H. K., MISHRA, R. S., RAMESH, V., WILFRED, D. and NATH, I. Effect of recombinant interferon gamma administration on lesional monocytes/macrophages in lepromatous leprosy patients. Int. J. Lepr. 61 (1993) 259-269.
Reprint requests to Dr. Ganapati at the above address or FAX 91-22-522-3040.