- Volume 64 , Number 1
- Page: 15–25
A survey of leprosy impairments and disabilities among patients treated by MDT in burkina faso
ABSTRACT
Since 1990, Burkina Faso, a West African country, has carried out a national leprosy control program treating with WHO/MD T nearly 12,000 patients between 1990 and 1994. A sample survey of 600 cases among these patients showed that 29.8% were disabled cases. There was a predominance of males, older patients, the multibacillary form of leprosy, and former cases treated with dapsone before MDT. The actual rate increased 8.5% compared to the frequency of disabilities at detection (21.3%). The need for disability care was estimated, respectively, at 24.4% and 5% for primary and secondary grades of disability. These important needs were so great that the authors recommend the planning and initiation of a physical rehabilitation and disability prevention program in this country.RÉSUMÉ
Depuis 1990, le Burkina Faso, un pays d'Afriquc occidentale, a realise un programme national de lutte contre la lèpre, traitant par PCT/OMS pros de 12.000 malades entre 1990 et 1994. Une enquête par échantillonnage de 600 cas parmi ces patients a montré que 29.8% d'entre eux étaient porteurs d'incapacités. Il y avait une prédominance d'hommes, de patients âgés, de forme multibacillaire de lèpre, et de cas traités antérieurement par dapsone avant la PCT. Le taux observé était plus élevé de 8.5% par rapport à la fréquence des incapacités à la détection (21.3%). Les besoins de soins pour incapacités ont été estimés à respectivement 24.4% et 5% pour les incapacités de grade I et II. Ces besoins étaient si grands que les auteurs recommandent la planification et la mise en route d'un programme de réhabilitation physique et de prévention des incapacités dans le pays.RESUMEN
Desde 1990, Burkina Faso, un país Africano occidental, ha implementado un programa nacional de control contra la lepra consistente en el tratamiento con PQT/OMS, de casi 12,000 pacientes entre 1990 y 1994. Una exploración de 600 casos entre estos pacientes mostró que el 29.8% fueron casos discapacitados. Hubo un predominio de hombres, de pacientes viejos, de la forma multibacilar de la lepra, y de casos tratados con dapsona antes de instituirse la PQT. La frecuencia de incapacidades aumentó en un 8.5% en comparación con la frecuencia encontrada al momento de su detección (21.3%). Se calculó la necesidad de atención de las incapacidades en un 24.4% y en un 5%, para los grados primario y secundario de incapacidad, respectivamente. Estas necesidades fueron tan grandes que los autores recomiendan la plancación y la iniciación de un programa de rehabilitación física y de prevención de las incapacidades en este país.Burkina Faso, a West African country, has elaborated and carried out a National Leprosy Control Program (NLCP) since 1989 (Ministère de la Santé et de l'Action Sociale Burkina Faso. Programme National Lepre-Tuberculose, Volet lutte antilepreuse, Dec, 1989). In this control program, treatment of leprosy cases consisted essentially of multiple drug therapy (MDT) recommended by the World Health Organization (WHO). Between 1990 and 1994, this MDT program treated nearly 12,000 persons, two thirds of whom had received dapsone monotherapy. Thus, leprosy registered prevalence considerably decreased during this period from 13,000 to 2000 cases (11). However, in this population treated by MDT, thousands of patients had leprosy impairments either existing at the time of detection or occurring during the treatment. The information system set up with the NLCP did not allow us to estimate the number of disabled cases nor to evaluate the need for disability care (Ministère de la Santé et de l'Action Sociale Burkina Faso. Rapport d'évaluation per opératoire de la lutte antilepreuse au Burkina Faso realise par A. S. Diallo, Consultant OMS, Dec. 1991 and Rapport d'évaluation du Programme National Lèpre du Burkina Faso. Travail conjoint Gouvernement/OCCGE/OMS, Mai, 1993).
The only leprosy hospital existing in the country is well equipped but was not operational due to the absence of trained staff and the lack of a physical rehabilitation program. That is why this survey was conducted in collaboration between the NLCP of Burkina Faso and the Marchoux Institute, a research and training center on leprosy in West Africa. The aims of the survey were to: a) estimate the frequency of impairments and disabilities due to leprosy among patients treated by MDT in Burkina Faso; b) evaluate the needs for the care of leprosy disabilities among these patients; and c) contribute to the planning for the activities for physical rehabilitation and disability prevention in this country. (In the following text, we have used alternately the terms "impairment" or "disability" to designate eye and nerve damage due to leprosy which could result in a "handicap" as described by Srinivasan10).
MATERIALS AND METHODS
Burkina Faso is a sub-Saharan country of 274,000 sq. km. with a population of 10 million. It is divided into 30 provinces, and the national health system is organized according to that administrative division. In each province a medical officer and a nurse specialized in leprosy control arc in charge of the NLCP application. Information on leprosy patients is available in the following documents kept at that level: leprosy registers, MDT booklets, and leprosy clinical forms.
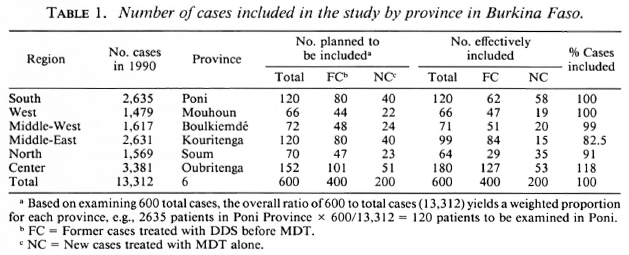
For this survey on leprosy disabilities, we decided to visit six provinces and to examine 600 patients treated with MDT between 1990 and 1995. To choose the six provinces, we clustered the 30 provinces of the country into six geographical regions of five provinces each (Fig. 1). In each geographical region, we chose the province with the greatest number of leprosy cases in 1990. The number of leprosy patients in the region decided proportionally the number of patients to be examined in each province (Table 1).

Fig.1. Map of Burkina Faso showing the six prov-inces visited. 1 = Poni, 2 = Mouhoun; 3 = Boulkiemde; 4 = Kouritenga; 5 = Soum; 6 = Oubritenga;- = country boundary; - = regional boundaries; - - - = provincial boundaries;  = province visited.
= province visited.
A month before the survey, we sent a calendar of the survey to the six provinces. The medical officer of each province selected randomized areas which allowed us to reach the number of patients of the local sample. Nurses informed leprosy patients of these areas to stay at home or to gather in the treatment centers during the survey day in their area.
During the survey, we collected information on patients and leprosy disabilities existing at the time of detection from leprosy registers, treatment booklets or the patients' clinical forms. We used a questionnaire to record information (Fig. 2, part one). We confirmed these data by interrogation of the patients found during the field visit. For actual disabilities due to leprosy, we obtained information by examination of the patients during the visit. In our sample we included 46 patients with recorded information on impairments at diagnosis and who were missing during the review. Information on actual disabilities of these patients was not available.
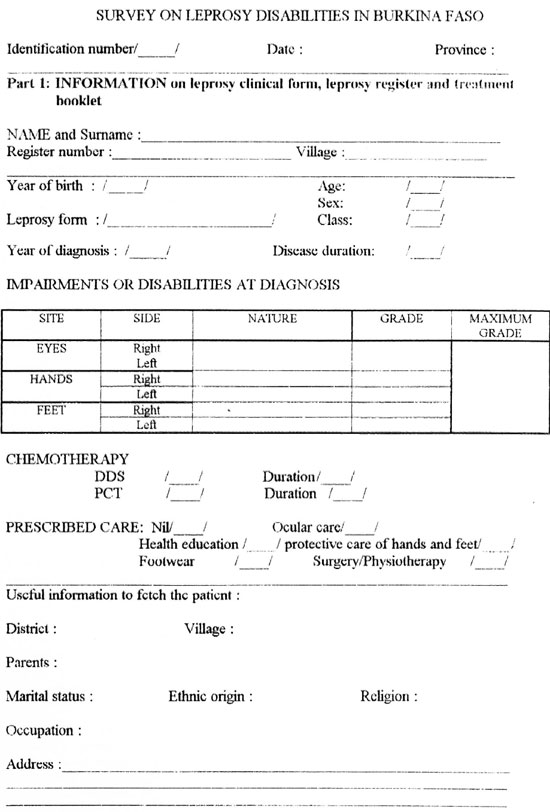
Fig. 2. Questionnaire form used during the survey.
The physiotherapist of the survey team practiced sensory and muscle tests on eyes, hands and feet of those patients seen. He used a ballpoint pen for sensory testing on the hands and feet as usually practiced by nurses at the time of diagnosis. We used the WHO scale of 1988 in three grades (0, 1, 2) to score the disabilities (12). According to the nature of the impairments, we evaluated the needs for disability care during examination of the patients in the field. Two classes of care grouped these needs: a) primary care that could be delivered by nurses in common health centers, including health education, training in skin and deformity care of hands and feet, delivery of protective means (footwear, gloves, sunglasses), noncomplicated ulcers treatment; and b) secondary care to be delivered by physicians or physiotherapists in equipped health centers: complicated ulcer care, training in lid strengthening, excision or salvage surgery, reconstructive and palliative surgery with preoperative and postoperative physiotherapy. All patients in need of secondary care also required primary care. For reconstructive or palliative surgery, all indicated patients were not real surgery candidates but needed to be reviewed by a surgeon for possible treatment. Information on actual disability and care needs was recorded on a questionnaire for each reviewed patient (Fig. 2, part two).
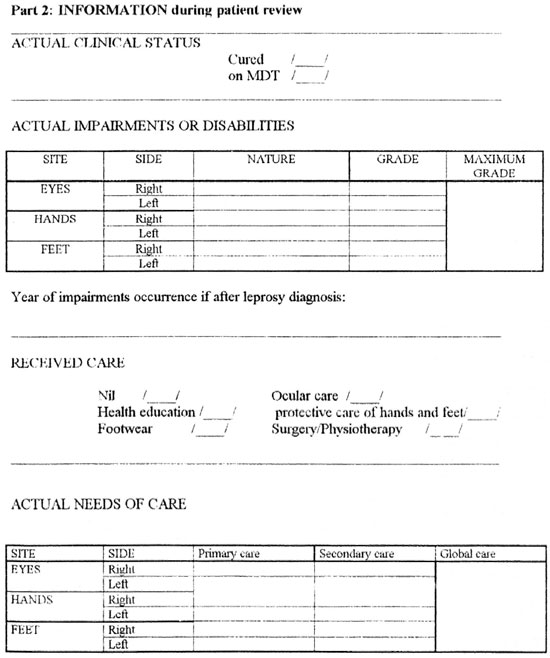
Fig. 2. Continued.
We used Epi-info software to analyze all of these data.
RESULTS
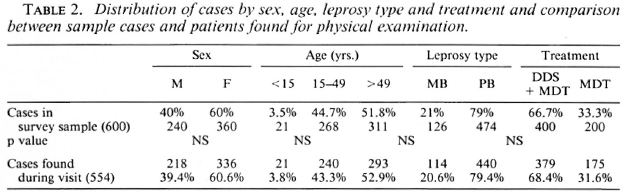
Characteristics of survey sample. In the sample of 600 patients, there was a predominance of females with 360 cases (60%). The average age was 47.9 years with a standard deviation of 16.2. Twenty-one percent of the cases were multibacillary (MB) patients and 67% were former cases of leprosy treated by dapsone (DDS) before MDT. During the field visit, we found 554 cases for examination among the 600 cases included in the study. The 46 missing patients had either died or were absent from their village during our visit. The differences between the sample of 600 cases and the 554 patients reviewed during the study were not significant for the frequency distribution by the different variables (Table 2). This allowed the comparison between disabilities at detection time and actual disabilities without a previous adjustment. The distribution of the sample by type of leprosy and by treatment received was similar to the entire leprosy case distribution in Burkina Faso. This allowed extrapolation of our results for all leprosy cases treated by MDT in this country.
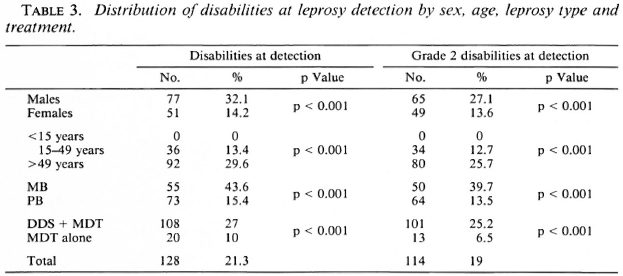
Disabilities at time of detection. Among the 600 cases of the sample, the frequency of impairment was 21.3% with a 95% confidence interval (CI) between 18% and 24.6%. Considering grade 2 disabilities, the frequency was 19% with a 95% CI between 17.5% and 20.5%. The frequency distribution of disabilities by sex, age, type of leprosy and treatment showed a predominance for males, older patients, MB form and former cases treated by DDS before MDT, even after adjustment for other variables: a) males = 32.1% with disabilities compared to females (14.2%, p < 0.001); compared to females, the relative risk for males was 2.26. b) older patients = 29.6% for those >50 years, 13.4% for those between 15 and 50 years old and 0% for children < 15 years old (p < 0.001). c) MB patients = 43.6% with disabilities and a significant relative risk of 2.83 compared to PB patients (15.4%, p < 0.001). d) former cases (FC) previously treated by DDS = 27% with disabilities and a significant relative risk of 2.7 compared to new cases (NC) treated with MDT alone (10%, p < 0.001) (Table 3). This lower disability rate for new cases probably reflects improvement in case detection with more health personnel involvement in the leprosy control program since 1990.
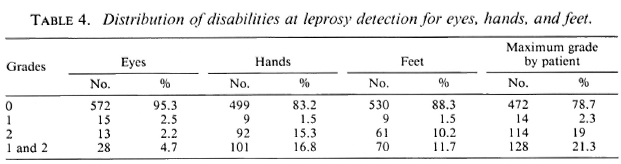
Disabilities due to leprosy were seen more frequently with hands (16.8%) than with feet (11.7%) and eyes (4.7%) (Table 4). Grade 2 disabilities were seen more frequently with hands and feet but less frequently with eyes. Among the 61 patients with grade 2 disabilities of the feet, 22 (36%) had planter ulcers and represented 3.7% of the sample cases.
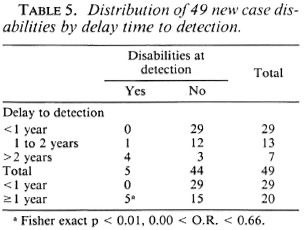
From clinical forms and patient questioning, we obtained reliable information on the detection delay (duration between first leprosy signs and leprosy diagnosis) for 49 new cases. Among those 49 patients, the frequency of disability was higher in cases with a longer detection delay. The odds ratio calculated for patients with < 1 year detection delay versus the others was 0.00 with exact confidence limits of 0.00 < OR < 0.66 (Table 5).
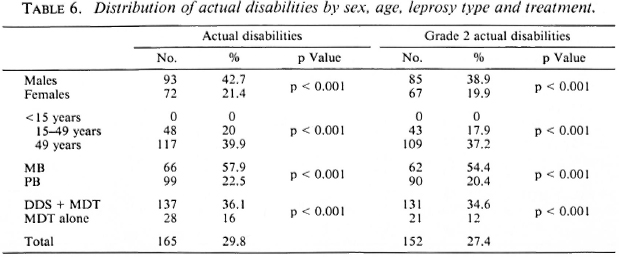
Actual disabilities (disabilities during field visit). Among the 554 cases examined during the field visit, the frequency of impairments was 29.8% with a 95% CI between 26% and 33.6%. The frequency of grade 2 disabilities was 27.4% with a 95% CI between 23.7% and 31.2%. The frequency distribution of disabilities by sex, age, type of leprosy and treatment showed the same predominance as disabilities at detection even after adjustment for other variables: a) males = 42.7% with disabilities and a significant relative risk of 1.99 compared to females (21.4%, p < 0.001). b) older patients = 39.9% for patients ±50 years old, 20% for those between 15 and 50 years old and 0% for children <15 years old (p < 0.001). c) MB patients = 57.9% with disabilities and a significant relative risk of 2.57 compared to PB patients (22.5%, p < 0.001). d) former cases (FC) previously treated with DDS = 36.1% with disabilities and a significant relative risk of 2.26 compared to cases treated with MDT alone (16%, p < 0.001) (Table 6).
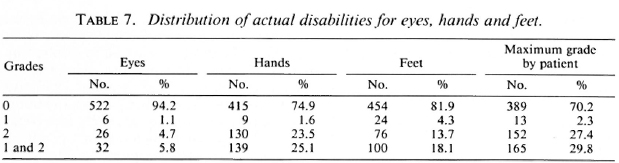
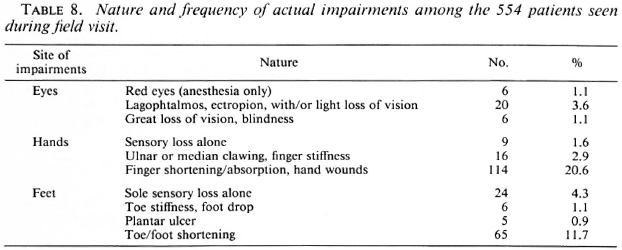
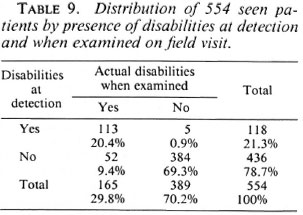
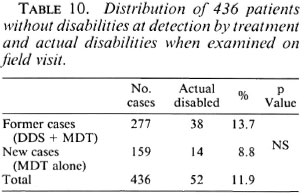
Actual disabilities were seen more frequently with hands (25.1%) than with feet (18.1%) and eyes (5.8%) (Table 7). Grade 2 disabilities were seen more frequently at all sites (eyes, hands and feet) and reached 92.1% of disabled patients. Actual plantar ulcers (five cases) represented 0.9% of examined patients (Table 8), but we noted that five patients with a plantar ulcer at diagnosis had salvage surgery and wore artificial legs; three other cases with an ulcer recorded on their leprosy forms were missing during the review. Only five patients with grade 1 disabilities at detection did not show actual impairment; 52 patients representing 11.9% of the nondisablcd cases at detection developed impairments (Table 9). Many former cases previously treated with DDS were found among the 436 patients who developed disabilities after detection (73%). However, their association with actual disabilities compared to cases treated by MDT alone was not significant (x2 test p > 0.05) (Table 10). The treatment received (DDS + MDT or MDT alone) did not seem to modify the risk of disability occurrence.
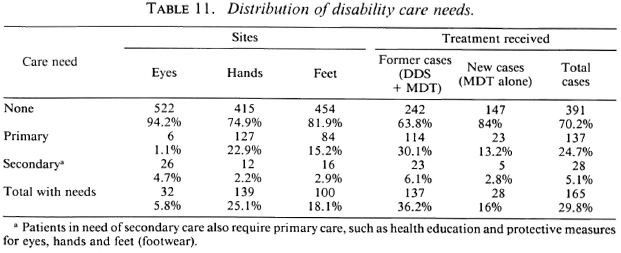
Disability care needs. The disability care needs were greater for hands (25.1% ofcases) than for feet (18.2%) and eyes (6.3%) (Table 11). Those in need of care were found more frequently among cases previously treated with DDS (35.9%) than those treated by MDT alone (15.4%). Primary care represented 82.8% of the needs and concerned 24.4% of the patients seen during the survey. Secondary care represented 17.2% of the needs for only 5% of the patients who were visited. Compared to the care received estimated by patient questioning (5.4%), all care needs (29.4%) were very important.
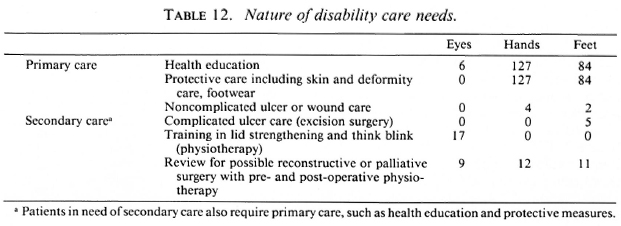
Health education of patients and their families and patient training for skin and deformity care were the most frequent needs forall patients with impairments (Table 12). Among secondary care, we counted only five complicated ulcers to be surgically treated. Five other cases of plantar ulcer were already cured by salvage surgery which could partially explain the small number of complicated ulcers found in the field.
DISCUSSION
Frequency of disabilities. The frequency of disabilities at detection in our study is near to those of Ponnighaus, et ai. in Malawi (7). Those authors found 20% of disabilities at detection for patients detected before 1980, and 10% of patients detected after the introduction of a population survey for leprosy. We also found a decrease in the disability rate at detection (10% among patients detected since 1990). This decrease was consecutive to the bettering of the health service coverage and more medical staff involvement in the leprosy control program with MDT. However, our results on disabilities at detection are not fully reliable, especially for the older patients, because they are based on document information and/or patient memory. In leprosy registers and clinical forms, descriptions of former cases' lesions at detection were often shorter than those of new cases. This mode of data collection could explain the very low number of plantar ulcers at detection in our study.
Another weakness of our results on actual disabilities was the verification of the leprosy diagnosis for patients seen during the survey. Most of them had finished their treatment and did not show any signs of leprosy. The frequency of actual disabilities in our survey (29.8%) is intermediary compared to other studies in the literature. In different papers disability proportion ranged from 10% to 60% (1,5-9). The great variation of the disability rate according to different studies is partially attributable to different definitions or classifications of disability and leprosy. In our survey, we considered some patients already cured and did not exactly follow the current WHO definition of a case of leprosy. Zhang, et al. in the Yangzhou Prefecture in China, found 56%-97% of cases with disabilities or deformities among 14, 257 leprosy patients (14). We did not take into account deformities of the face in our study.
The more frequent disabilities seen in males, older and MB patients were also found in other studies, and several reasons could explain these facts: longer delay for detection for men and MB patients, longer evolution of the disease in older patients, males working outdoors. These reasons probably explain the highest proportion of disabilities among cases treated with DDS before MDT. They were older and had a longer evolution of the disease than did patients treated with MDT alone. On the other hand, we found a low rate of plantar ulcers among patients examined during the survey (0.9%) compared to results found in neighboring countries [Benin = 7.3% among 5273 cases (3); Senegal = 5.3% among 190 cases (4)]. Perhaps the desert climate in Burkina Faso, very hot and dry, and the habit of walking without shoes since childhood in rural areas reduce the incidence of ulcers. A great majority of our cases had rough and thickened soles of their feet.
Extent of disabilities in Burkina Faso and care needs. Extrapolating our results to the entire number of leprosy cases treated with MDT in Burkina Faso (12,000), we could estimate the number of disabled patients at 3500. This number must be multiplied by three if we take into account living leprosy patients cured by DDS between 1980 and 1990 (nearly 30,000 cases). Thus, the number of patients needing disability care could reach 10,000, equaling a rate of 1 per 1000 of the country's total population. The number of patients in need of disability care is fivefold more numerous that those needing MDT. Physical rehabilitation and disability prevention must be added to the NLCP (12).
Among these disabled patients 5% (nearly 500 cases) would need treatment in a center equipped for surgery and physical rehabilitation. Giraudeau and Despinay (2) found the same results in 1979 among patients treated by DDS in a rural area of Mali (a neighbor country of Burkina Faso). The national leprosy hospital in Burkina Faso would be insufficient to face these needs for surgery and physiotherapy. Some general surgeons would need to be trained to deal with these needs in the regional hospitals of the country. Considering the number of disabilities occurring after detection, nurses in common health services must be trained in the early diagnosis of leprosy and neuritis and for disability prevention.
Acknowledgment. The authors would like to express their deep thanks to all who contributed to this survey: Association Française Raoul Follercau for its financial support, the Ministry of Health of Burkina Faso and the staff of the National Leprosy Control Programme, the physicians, nurses and nonmedical workers who participated in the field visits, and all leprosy cases who accepted examination by the survey team.
REFERENCES
1. COMPOSTELLA, L., CERRANO, A., BARACCA, G. and MACARTHUR, A. Prevalence of deformities in the leprosy patients in Mozambique. (Abstract) Int. J. Lepr. 61(1993)156A.
2. GIRAUDEAU and DEPINAY, J. Place et importance de la chirurie "spécialisée" dans un programme national de lutte contre la lepre. Med. Trop. 39(1979)57-579.
3. Ji, B. and GRAUWIN, M. Y. Les activités du programme national de lutte antilcpreuse du Benin sur la prevention des invalidités et la rehabilitation physique. Rapport de mission organisée par l'Association Française Raoul Follereau, 1993.
4. MANE, I. GRAUWIN, M. Y. and CARTEL, J. L. Frequence d'apparition des maux perforants plantaires chez des malades hanseniens en fonction du traitement par disulonc seule ou par PCT. Acta Leprol. 9 (1995) 127-131.
5. NOORDEEN, S. K. A look at world leprosy. Lepr. Rev. 62(1991)72-86.
6. NOORDEEN, S. K. and SRINIVASAN, H. Epidemiology of disability in leprosy; a general study of disability among male leprosy patients above fifteen years of age. Int. J. Lepr. 34(1966)159-169.
7. PONNIGHAUS, I. M., BOERRIGTER, G., FINE, P. E. M., PONNIGHAUS, J. M. and RUSSEL, J. Disabilities in leprosy patients ascertained in a total population survey in Karonga District, northern Malawi. Lepr. Rev. 61(1990)366-374.
8. RAO, P. S. S., KARAT, S., KARAT, A. B. A. and FURNESS, M. A. Prevalence of deformities and disabilities among leprosy patients in an endemic area. Int. J. Lepr. 38(1970)1-11.
9. SAHA, S. P. and DAS, P. K. Disability pattern among leprosy patients. Indian J. Lepr. 65(1993)305-314.
10. SRINIVASAN, H. Prevention of disabilities in patients with leprosy; a practical guide. Geneva: World Health Organization, 1993.
11. TIENDREBEOGO, A., BLANC, L. and SYLLA, P. M. La PCT antilepeuse dans les Etats de l'OCCGE; une décennie de mise en oeuvre (1983-1993). Acta Leprol. 9 (1995) 139-147.
12. WATSON, J. M. Disabilities control in a leprosy control programme. Lepr. Rev. 90 (1989) 169- 177.
13. WORL D HEALTH ORGANIZATION. A guide to leprosy control. 2nd edn. Geneva: World Health Organization, 1988.
14. ZHANG, G., LI, W., YAN, L., YANG, Z., CHEN, X., AHENG, T. and YE, G. An epidemiological survey of deformities and disabilities among 14, 257 cases of leprosy in 11 countries. Lepr. Rev. 64(1993)143-149.
1. M.P.H., Unite Epidemiologie-Formation.
2. Physiotherapist, Institut Marchoux, 13. P. 251, Bamako, Mali.
3. M.P.H., Manager, National Leprosy Program, Burkina Faso.
Received for publication on 28 July 1995.
Accepted for publication in revised form on 26 October 1995.