- Volume 64 , Number 1
- Page: 87–95
News and notes
This department furnishes information concerning institutions, organizations, and individuals engaged in work on leprosy and other mycobacterial diseases, and makes note of scientific meetings and other matters of interest.
1995 DAMIEN-DUTTON AWARD RECIPIENT
Dr. Joon Lew, 1995 Damicn-Dutton Award winner.
On 27 November 1995, Dr. Joon Lew, Director of the Lew Institute for Biomedical Research in Seoul, Korea, became the 1995 Damien-Dutton Award winner. The Award was presented to Dr. Lew by Dr. Wayne M. Meyers, Board Member of the Damien-Dutton Society. Dr. Meyers' presentation speech follows.
"This evening I have the distinct pleasure and honor on behalf of the Damien-Dutton Society of New York and its President, Mr. Howard E. Crouch, to announce the recipient of the Damien-Dutton Award for 1995, Professor Joon Lew, Director of the Lew Institute for Biomedical Research here in Seoul.
"The Damien-Dutton Society for Leprosy Aid and the Damien-Dutton Award are named for the heroic Belgian priest, Father Damien, who volunteered to go to the famous leprosarium on the island of Molokai, Hawaii, in 1873, and for the American layman, Brother Dutton, who went to Molokai to assist Father Damien in 1886. Both of these men had offered themselves so that they could bring hope to the hopeless and dignity to the downtrodden. Both drew the attention of the world to the plight of leprosy patients and to its stigma that, although ameliorated in many places, continues to this day around the world.
"It is interesting that in the same year that Damien went to Molokai-1873-another hero in the annals of the history of the science of leprosy made an astounding discovery. I speak of G. Armauer Hansen who, after years of careful study in Bergen, Norway, was the first to observe the leprosy bacillus and to recognize it as the cause of this disease.
"It has been said of Father Damien, the 'Holy Man of Molokai', that in him 'belief was unaffected, incarnate, and faith was made physical.' In a large sense, the life of the son of Korea whom we honor tonight can clearly be thought of in similar terms. He has effectively melded the humanitarian and spiritual concern of Damien and Dutton with the scientific inquiry of Hansen into a strong movement that in Korea and elsewhere has changed the image of leprosy and those whom it afflicts.
"In his 20s, while attending Seoul Medical College, Prof. Joon Lew began to see the abject poverty and misery of the leprosy patients in the community who were, more often than not, wandering and despised beggars. He says, in writings from his impressions as a physician just out of medical school and working at the Sorok Island Leprosarium, that that institution in the early 1940s was a '... strict segregation center, which was regarded as the most feared and hated hell to the patients ...' From this he observed that '... compulsory segregation was not only inhumane but unscientific.' Prof. Lew further noted that although these unfortunates ( 'Les miserables' ) had no resources, 19 out of 20 of these outcasts were physically fit. He saw this and ingeniously set about to change the face of leprosy in Korea, both the medical aspects and the social issues. The former had a rational scientific solution -look for a medical cure for the disease and rehabilitate the physically disabled, and for the latter he proposed to 'unite the labor power to support themselves ... and provide some financial benefit to the country.'
"Following graduation from medical school and obtaining a Doctorate of Medical Sciences at KyuShyu University in Japan, Prof. Lew was instrumental in founding the Korean Leprosy Association in 1948, and served as its President and Chairman of the Board. He encouraged the leaders of the patients to form the Sang-Ju Society (Mutual Help Society), now known as the Hansung Cooperation Association. The Hope Village Movement was organized at this time and by 1950, 5000 leprosy patients were being cared for and caring for themselves in these villages where the mind-set was that they were no longer beggars but were self-supporting workers and were helping others. Beginning with second-hand tools and donated resources, the resettlement villages of patients were managed by the residents and engaged in shared industries of highly diversified kinds-from pig and poultry raising to the manufacture of industrial materials.
"While these operations were disastrously interrupted by the conflict of the early 1950s, afterward they were re-established and enlarged, particularly following a countrywide survey of some 20,000 leprosy patients who were given the opportunity to join the Resettlement Village Movement. Prof. Lew was influential in engaging governmental and philanthropic support initially, but before long the patients themselves were becoming highly successful business people. For example, the products of these resettlement villages now comprise 30% of the poultry market in Korea. Today many of these villages have become normal unsegregated villages, the patients suffer virtually no discrimination in public or in marketing their products, nor in obtaining education for their children. All of these accomplishments arc a great credit to the vision, energy and genius of Prof. Lew, and have become models for other societies with similar problems.
"In addition to all his direct patient-oriented activities, Prof. Lew was a pioneer in medical education and research. After obtaining his Doctor of Philosophy degree in Infectious Diseases at the University of California at Los Angeles, he began a career in academia as Professor and Chairman of Microbiology and Dean of the College of Medicine at Yonsei University. He also was President of Ycungnam University for several years. In addition to being Director of the Lew Institute for Biomedical Research, he is now Chairman of the Board of Trustees, Taeshin University.
"Prof. Lew's research has produced more than 200 scientific articles in domestic and international journals, and his other writings include textbooks on leprosy and microbiology, an autobiography, and a monograph entitled, A Model for Healing of Leprosy in Korea.
"Prof. Lew's work in establishing the Korean chipmunk as a model for studying the disease of leprosy is of particular interest to me and over the last few years has attracted the attention of others interested in experimental leprosy.
"In various capacities Prof. Lew has served or is serving many organizations involved in the worldwide struggle against leprosy. Among these are: Korean Association of Leprologists, Korean Association of Leprosy Service Organizations, Korean Leprosy Control Association, and the International Leprosy Union.
"Honors and recognitions for Professor Lew's leadership have included: the Culture Order for the National Public Service from the Republic of Korea (1962), the May 16 National Award in the Academic Field from the President of the Republic of Korea (1969), the Award for Distinguished International Cooperation and Leprosy Research at the Leprosy Mission Centenary in London ( 1974), and the Elise and Walter A. Haas International Award of the University of California (1987).
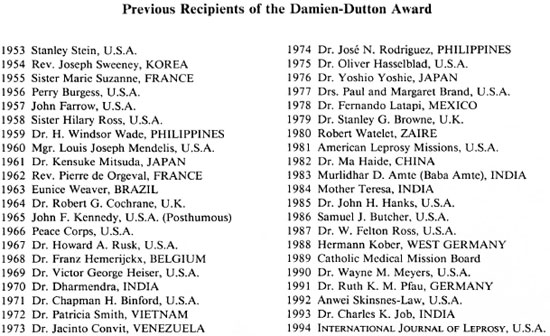
"Ladies and gentlemen, tonight I am proud to present to Prof. Joon Lew the Damien-Dutton Award for 1995. In receiving this recognition, he joins a group of wellknown leprologists and humanitarians who, for approximately three-quarters of a century, have fought the good light to bring healing and happiness to those afflicted with leprosy. Among these names are Doctors Mitsuda, Dharmendra, Cochrane, Binford, Browne, Paul and Margaret Brand, and Mother Theresa. John F. Kennedy was honored posthumously for his official declaration of World Leprosy Day in my country.
"The citation for this award acknowledges in succinct terms Prof. Lew's contributions:
1995 DAMIEN-DUTTON AWARD
presented to
DR. JOON LEW, M.D., PH.D.,
FOR HIS LLFE-LONG CAMPAIGN OF THE
HEALING OF LEPROSY, FOR HIS
COMPASSION FOR THOSE WH O BEAR THE
STIGMA OF THIS DISEASE
AND FOR THE ESTABLISHMENT OF THE
RESETTLEMENT VILLAGE MOVEMENT WHICH
BRINGS HOPE AND RESTORED DIGNITY TO
THE PATIENTS AND THEIR FAMILIES
THROUGHOUT SOUTH KOREA
"Prof. Joon Lew, the Damien-Dutton Society for Leprosy Aid is proud to honor you and, through you, all those who have struggled with you and who have benefited from your vision and leadership. I wish to add my personal heartiest congratulations and best wishes."
Hong Kong. International Congress for Infectious Disease. The 7th International Congress for Infectious Diseases will be held 10-13 June 1996 in Hong Kong. For details contact: International Society for Infectious Diseases, 180 Longwood Avenue, Boston, MA 02115, U.S.A. (FAX = 1-617-731-1541).
India. ALH RRE Society holds seminar. Under the joint auspices of Acworth Leprosy Hospital, Society for Research, Rehabilitation and Education in Leprosy, Wadala, Bombay, and the Vocational Rehabilitation Centre (VRC) for Handicapped, Sion, Bombay, a seminar on "New Dimensions in Rehabilitation of Persons with Leprosy-Community Based Rehabilitation" was conducted on 6 December 1995 as the celebration of World Disabled Day. Representatives of antileprosy agencies (13), institutes working for disabled person (25) and social organizations (4) from Bombay attended the seminar. Mr. S. S. Naik, Hon. Secretary, ALH RRE Society, explained the objects of the seminar as understanding, initiating and strengthening existing community-based rehabilitation programs for leprosy-disabled persons with the help of nonleprosy agencies and the community. The following experts presented their work in rehabilitation of leprosy: Dr. C. R. Revankar, Deputy Director, Bombay Leprosy Project (BLP), spoke on medical rehabilitation of leprosy; Mr. T. P. Mirajkar and Mr. Kingsley from BLP highlighted their leprosy rehabilitation work in Bombay and other states; Mr. R. Narasimham, Sr. Superintendent, VRC, gave a review of the last 10 years work of his center under the title "Community-based Vocational Training (CBVT)." Dr. S. P. Gudi from the Regional Rehabilitation Training Centre explained the concept of community-based rehabilitation and narrated their experiences in a rural area in Thane District. Mr. S. G. Joshi, community development officer, ALH RRE Society, gave a short review of his experience of prevention of dehabilitation of leprosy-suffering children through a child sponsorship program and an income generating scheme for women leprosy patients through self employment. The discussion was moderated by Mr. Narasimham, Sr. Superintendent of VRC, and ably supported by Dr. Ganapati, BLP Director, with his valuable suggestions.
It was felt strongly that efforts should be made to collect proper data on disabled persons along with leprosy-disabled persons on a district level and, as a model, work out a proper strategy for community-based disability care (CBDC) with community-based vocational training (CBVT). It was further observed by the participants that community awareness at different levels and the systematic device of outreach service of referral centers have to be jointly worked out for community-based rehabilitation. The general impression derived from the discussion was that the exercise of community-based rehabilitation in our country is still at the infancy stage and a lot of work on different facets of it has to be carried out. The vote of thanks were proposed by Dr. (Mrs.) Momanty, psychologist from VRC.
The following recommendations have been formulated by the group regarding community-based rehabilitation in leprosy.
1. Community awareness as a whole is required to understand the problems of the disabled, i.e., leprosy cured and other categories of disabled both ways.
2. Need for community-based disability care (CBDC) with community-based vocational training (CBVT) and favorable support of the local agency is jointly required for community-based rehabilitation.
3. Health care workers and field attendants may be made accountable to the patients in the community.
4. Community support is required in the form of social acceptance of disability.
5. Need of closer coordination with the organizations with leprosy and other disability groups is required for the outreach rehabilitation program.
6. The work for formation of cooperatives for leprosy to initiate cured persons with other disability groups is required in urban and rural areas.
7. Voluntary organizations for leprosy can collect the data on disabled persons in their operational area along with leprosy-disabled persons and initiate community-based vocational training with the collaboration of a vocational rehabilitation center.
8. An urban referral center and routine health service components which are important parts of the community may be involved in community-based rehabilitation.
9. To help the poor and poorly informed community, the local resources, local agencies, financial institutions, banks or philanthropic clubs may be invited to collaborate in community-based rehabilitation.
10. Need is felt to motivate the staff practicing in institutional rehabilitation to community-based rehabilitation and also the local community as a whole is required to be motivated.
11. Parents of disabled community members may be educated with special emphasis on disabled children to rehabilitate in family and community. -Materials from S. S. Naik.
BLP enters 20th year of research. Dr. A. R. K. Pillai, President, Indian Leprosy Foundation, who was the Chief Guest of the 19th Anniversary function of the Bombay Leprosy Project (BLP) on 6 October 1995, applauded the assistance offered by the project to the National Leprosy Eradication Programme through its outstanding research contributions over the last two decades. He recalled the difficult teething periods in the initiation of the Project's work which has culminated in offering a novel path for "low cost medical and disability management of leprosy."
Dr. C. R. Revankar, Deputy Director of BLP, exhorted the large gathering of project staff to dedicate itself to the proposed tuberculoses (TB) work in the future which has been taken on as a policy decision in view of the decline in the leprosy caseload as a result of dedicated work by the staff.
Dr. R. Ganapati, BLP Director, who had to attend a crucial meeting of Bombay Municipal Corporation and World Bank authorities in order to champion the credibility of the project to take up TB work in the largest slum in Asia (namely, Dharavi) and thereby offer security to the staff through his message announced that the project will bring out a consolidated publication of its contributions over two decades on the 20th Anniversary in October 1996.
Mr. P. Narayanaswamy, BLP Manager, proposed a vote of thanks. -Materials from R. Ganapti
Changing concepts in leprosy treatment. A lively discussion among health officials, clinicians, paramedical professionals, etc., on the strategies needed to reorient the medical professionals, particularly dermatologists, on modern short-course chemotherapy followed a presentation on the subject of "Newer drugs in Leprosy" by Dr. Ratna, dermatology lecturer of the LTM Medical College (LTMMC), Sion. The occasion was an academic meeting organized by the Research Society of Acworth Municipal Leprosy Hospital on 15 October 1995 as part of the Society's 25th year celebrations.
The crucial role of the newly formed Maharashtra Branch of the Indian Association of Leprologists in undertaking this challenging task was stressed by Dr. R. Ganapati, Director, Bombay Leprosy Project. Dr. (Mrs.) P. R. Vaidya, Dean of LTMMC and the chief guest, pointed out that the excellent model existing in the college for updating postgraduate students and staff effectively in the recent advancements in leprosy chemotherapy should be replicable. Mr. S. S. Naik, Secretary of the Research Society, moderated the proceedings and proposed a vote of thanks. -Materials received from R. Ganapati
CLT&RI 1994-1995 Annual Report. We have received a copy of the Annual Report 1994-1995 of the Central Leprosy Teaching and Research Institute (CLT&RI), Chengalpattu. We quote from the Foreword by Dr. P. S. Rao, Director-in-Charge:
"During this year some of the notable achievements were: i) Movement of training faculty members to outside the institute and organisation of a training workshop at Bangalore on 'Managing Programmes for Leprosy Control' by which 24 district and state level officers of Karnataka State were trained in the managerial aspects of leprosy control work with assistance from WHO. ii) Commencement and intake of about 331 cases of leprosy into the WHO-sponsored, multicentric, double-blind field trial of 'Treatment of single lesion Paucibacillary leprosy cases' with single-dose MDT. iii) Commencement of study on 'Integration of leprosy control activities of vertical nature with PHC services' in two selected districts of Andhra Pradesh which is supported by ICMR. iv) Acquisition of a video projector to facilitate training programmes and v) Acquisition of a coulter MD-8 and its accessories-Haematology analyser.
"Though vacancy of group A posts, in specific specialist posts, to the extent ofabout 50% continued throughout the year, about 20 research projects were pursued vigorously with the active participation and cooperation of all the stall" in various divisions of the institute."
Devikaran receives Gayatri Award for 1994-1995. The Gandhi' Memorial Leprosy Foundation (GMLF), Wardha, has announced that Mrs. Girija Devikaran,-Non-Medical Supervisor (NMS), Bombay Leprosy Project (BLP), will be the recipient of the Gayatri Award for 1994-1995 for excellent work in the field of leprosy. This yearly Award, which was instituted by GMLF in 1990 to recognize the merit of trained paramedical field staff of at least 15 years' experience consists of Rs. 10,000 in cash and a citation. Mrs. Girija will receive the Award on 1 January 1996 in Wardha.
It is significant that Mrs. Girija is the second BLP field worker to be honored, the first recipient of the Gayatri Award being Mrs. Rashmi R. Pai, NMS, for 1990-1991.
In the context of gender issues relating to leprosy patients as well as workers currently being seriously discussed by leprosy experts all over the world, the fact that female workers are recognized in this manner is a happy augury for the future of leprosy work, with the target year for elimination of the disease in the country being 2000 A.D. -From materials from R. Ganapati
Japan. International Epidemiological Association to meet. The 14th international scientific meeting of the International Epidemiological Association: Global Health in a Changing Environment will take place 27- 30 August 1996 in Nagoya, Japan. For information contact: Conference Secretariat, c/o Department of Preventive Medicine, Nagoya University School of Medicine, 65 Tsurumai-cho, Showa-ka, Nagoya, 466, Japan (TEL = 81-52-7412111, ext. 2074; FAX = 81-52-7336729).
Japanese Leprosy Association resolution. The most recent Congress of the Japanese Leprosy Association (JLA) resolved to support abolition of the Absolution Act for Compulsory Segregation of Hansen's Disease Patients, an unscientific and inhumane law still in effect in Japan.
The Committee for Examination of the Leprosy Prevention Law organized by the JLA reported its views concerning this law to the President of the 68th JLA Congress, H. Nakajima, M.D., Professor, Department of Dermatology, Yokohama City University School of Medicine, on the first day of the Congress which was held 22 and 23 April 1995 in Yokohama City. The Committee report was accepted by the Congress participants.
The fundamental means of dealing with Hansen's disease (HD) in Japan is by segregation of patients into specialized medical institutions, and the Prevention Law has played a major role as the legal basis for this segregation. The Committee concluded that, based on epidemiological findings, the decrease in the number of patients with HD in Japan might be due mainly to improvement of living standards and might be unrelated to the exclusion of sources of infection from the community. It was, therefore, concluded that the continuation of the Prevention Law aiming at absolute segregation of possible sources of infection is unnecessary.
Japan selected the above method of enforcement of absolute segregation because it was thought that, although the infectivity of HD is extremely weak, every patient had the potential to cause infection at home where repeated contact with family members was possible. In addition, HD was misunderstood to be incurable once its onset had occurred.
Further, the social conditions in Japan in 1930, when absolute segregation was the desired goal, were strongly affected by a highly nationalistic political climate which led to the belief that H D and affected patients were a disgrace to national prestige, and also to the doctrine of social defense, justifying segregation.
Even though the original Prevention Law (established in 1907 in Japan and aimed at absolute segregation) was revised three times, the existing law (established in 1953) invariably supports the fundamental principle of segregation, while by 1953 the clinical effect of Promin® had already been manifested and the usefulness of segregating HD patients was being denied internationally.
Despite the trend of the times, the reason the existing Leprosy Prevention Law has not been abolished until now is that 90% of the patients had already been segregated by 1953, while the number of new cases since then has drastically decreased and some previously segregated patients could return to the community over a period of years since 1953. As a result, compulsory segregation has become less strictly enforced, and ambulatory treatment gradually has been favored. Thus, the interest in the Prevention Law among staff members of leprosaria has spontaneously weakened.
The JLA has not taken the initiative in abolishing the existing law, nor has it been able to correct errors in measures dealing with HD in Japan. In the name of the JLA Congress, we regret that we have tacitly permitted the long-term continuation of the existing law. The measures required for dealing with HD are, needless to say, medical in nature.
Concerning measures to be taken following abolition of the existing law, it is strongly hoped that a life of ease and comfort may be guaranteed every inpatient in the future, including even financial compensation. Since the average age of inpatients is over 71, while the life of citizens in the main cities of Japan is comparatively hard, and since there is liable to be prejudice against HD, it is desirable that leprosaria be maintained as medical institutions practicing protective care for affected patients. Since HD symptoms, including those of the reactional phase, peripheral neuritis and iridocyclitis, are now controllable, and since new cases will therefore be treated principally as outpatients, application of health insurance to the treatment of HD at ordinary hospitals is urgently needed. In addition, in view of the fact that whole body clinical care is indispensable to the treatment of HD, it is hoped that suitable general hospitals will function as clinical bases for treatment of HD patients and will endeavor to educate staff capable of treating HD and even specializing in HD.
Reflecting on the past, when compulsory segregation and the Prevention Law were enforced, it becomes clear that the existing law should be abolished. Through these endeavors, the Japanese Leprosy Association will be able to grow out of its internationally isolated state into the international HD field.
- Japanese Leprosy Association
Committee for Examination of the
Leprosy Prevention Law
Chairman: Minoru Narita, M.D.
JLA General Affairs Secretary
Committee Members: Eiji Nagao, M.D.,
Masanao Makino, M.D.,
Masamichi Goto, M.D.
and Motoaki Ozaki, M.D.
Translator: S. Tsutsumi, Ph.D.
Tropical Medicine and Malaria congress to be held. The 14th International Congress for Tropical Medicine and Malaria is scheduled for 17-22 November 1996 in Nagasaki, Japan. Contact: Dr. Keizo Matsumoto, 14th Congress of Tropical Medicine and Malaria, c/o Institute of Tropical Medicine, Nagasaki University, 1-12-4 Sakamoto, Nagasaki 852, Japan (TEL/FAX = 81-958-432194).
Switzerland. e-Mail for TDR. TDR has set up an e-mail distribution list which is called (TDR-SCIENTISTS @who.ch). The list is used for announcements from TDR and can also be used for electronic discussion. It is open to anyone connected to Internet via e-mail. Interested readers should send a subscription message to: (TDR SCIENTISTS-REQUEST @who.ch). For those already on full-node Internet, all the latest public documents and data from TDR can also be accessed through (gopher.who.ch).
Report of first meeting of WHO LEAG. The Conclusions and Recommendations of the Report of the First Meeting of the Leprosy Elimination Advisory Group (LEAG), meeting in Geneva on 12 and 13 July 1995 are as follows:
"The Leprosy Elimination Advisory Group (LEAG) reviewed the progress being made towards the elimination of leprosy through the implementation of multidrug therapy (MDT) at the global and regional levels. The Group was encouraged by the steady improvement in the global leprosy situation. However, it expressed its concern with regard to the relatively slow progress in a few countries as it appeared from the reports submitted. While the elimination goal aims at a prevalence below 1 case per 10,000 population, countries should aim at reaching this target at national and sub-national levels.
"Since late detection of cases remains a problem in a number of countries and MDT implementation appears to be slow in some places, the Group recommended developing in those places special reinforcing campaign approaches based on specifically targeted activities, which however would not be a substitute for current approaches through the general health services.
"The LEAG considered that the task forces on Capacity Building and Health Systems Research (CBH) and on Monitoring and Evaluation of Elimination of Leprosy (MEE) and the steering committee on Special Action Projects (SAPEL) are appropriate for reviewing the situation and taking appropriate decisions.
"The LEAG supported the further expansion and continuation of the management training modules, which have contributed greatly to improving leprosy services in many endemic countries. It recommended that leprosy be included in the curricula of medical schools and other schools for health professionals, especially through the development and provision of task-oriented learning materials appropriate for different levels. It also is recommended that Health Systems Research (HSR) be used as an important component in capacity building, but from the lessons learnt it was clear that HSR should be oriented to problem-solving at the local level.
"Essential Indicators for Monitoring and Evaluating elimination identified earlier are sufficiently reliable and should continue to be limited to six; it is important that they be analysed at sub-national level. The LEAG recommended that additional indicators, namely incidence, disability, relapse and defaulting, be monitored in selected projects.
"SAPEL is a welcome innovative approach to addressing special situations and difficult-to-rcach patients which cannot be quickly dealt with through the routine health services. It is recommended that this initiative should develop in close collaboration with all possible partners.
"The LEAG welcomed and endorsed WHO's Guide to Eliminating Leprosy as a Public Health Problem as a timely publication, and strongly recommended its widespread distribution.
"Early treatment with MDT is the most effective way of preventing disabilities. The WHO gradings of disability are useful for monitoring early detection, and there is a need for new approaches to assessing disabilities and handicaps due to leprosy. Simple and cost-effective action for the prevention of disability by patients, health staff and communities should be promoted and complemented.
"Current research confirms the ellicacy of WHO fixed-duration MDT. It is important to ensure adequate supply and distribution of the MDT drugs, which have been made possible through the generous support from the Sasakawa Foundation.
"The LEAG emphasized that the present window of opportunity resulting from global political commitment, the provision of financial support for drugs and the scientific and technological breakthrough should not be lost. However, it should not be overlooked that elimination as a public health problem has not yet been achieved and further intensive efforts are needed. There is a risk of relaxing the required efforts, and steps must be taken to maintain the momentum at all levels, in close collaboration with different partners. The Group emphasized that, in the later phase of elimination, leprosy expertise must continue to be maintained at appropriate levels.
"The group recommended that, in view of the important need for sharing experiences, reinforcing commitment, reviewing progress and maintaining momentum towards elimination, the next International Conference on the Elimination of Leprosy should be organized before the end of 1996 as a follow-up to the Hanoi Conference of 1994."
U.S.A. ALM international conference on leprosy. The American Leprosy Mission (ALM) will hold an international conference on leprosy 6-12 April 1996 at Carville, Louisiana. For details contact: Dr. W. Felton Ross, ALM, 1 ALM Way, Greenville, SC 29601.
American Leprosy Missions appointments. In January 1995 Christopher J. Doyle became President and Chief Executive Officer of American Leprosy Missions (ALM International). He is responsible for using all available resources-MDT, vocational programs, clinic support, healthworker training, rehabilitation and physical therapy- to direct ALM's ministry in a way that will rebuild broken lives and restore the dreams that all parents have for their children's future. Mr. Doyle is only the twelfth person to lead ALM's worldwide campaign against leprosy which began in 1906 and supports programs in 30 countries, providing medicine, rehabilitation, and Christian encouragement to people with leprosy.


Also in 1995, M. Dennis Brown was appointed to the position of Chief Development Officer of ALM. He will manage ALM's fundraising and donor development activities.

In 1966 Lance Renault was appointed as ALM's Chief Program Officer with overall responsibility for ALM's leprosy treatment and rehabilitation projects around the world.
Leprosy 1994. A total of 136 new leprosy patients were diagnosed in the U.S. in 1994. Forty-three cases were reported from California, 31 from Texas, 21 from Hawaii, and 15 from New York.- MMWR 43 (1994)