- Volume 64 , Number 2
- Page: 177–83
News and notes
This department furnishes information concerning institutions, organizations, and individuals engaged in work on leprosy and other mycobacterial diseases, and makes note of scientific meetings and other matters of interest.
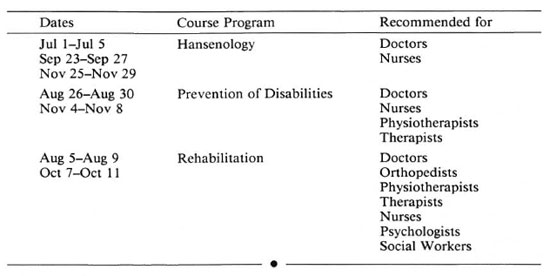
Brazil. 1996 Training calendar at Bauru. The following training courses are planned for the rest of 1996. Courses are in Portu-guese; lodging is available at the Institute.Fees: 1-week course = US$10; 2-week course= US$20 inscription fee; per diem US$3 (meals included). For further details contact: Dr. M. Virmond, Chief of Training Section, Institute Lauro de Souza Lima, Rodovia Cte. Joao Ribeiro de Barros, KM225/226 Bauru, SP, 17100 Brazil. Tel: 55-142-30-2244; Fax: 55-142-30-4747.
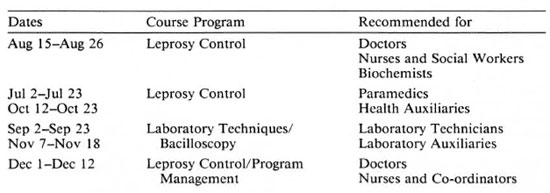
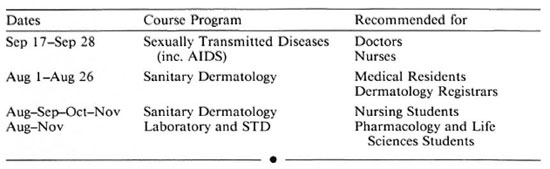
1996 Training calendar at Manaus. The following training courses are planned for the rest of 1996. Courses are in Portuguese and Spanish. For further details contact: Dr. M. G. S. Cunha, Head of Training Unit, Alfredo da Matta Institute for Tropical Dermatology, Rua Codajas, No. 25, Cachoeirinha, Manaus 69065-130 AM, Brazil. Tel: 55-92-663-2350; Fax: 55-92-663-3155.
India. 1996 International Gandhi Award to Jean Watson. The Bombay Leprosy Project (BLP) had the proud privilege of honoring the recipient of the International Gandhi Award for 1996 Ms. Jean Watson, an eminent physiotherapist, from the U.K. on 3 February 1996.
Dr. Ganapati, Director of BLP, while introducing this recipient said that recognition of the monumental contribution of Ms. Watson is a turning point in the history of our march toward the goal of total eradication of leprosy which includes the important component of physical care of the leprosy-afflicted due to nerve damage besides implementing strategies governing the arrest of the transmission of the disease. However, a consensus on policies in respect to field care of patients is yet to be evolved in the country.
Dr. A. R. K. Pillai, President of Indian Leprosy Foundation (ILEF), congratulated Ms. Watson on behalf of BLP and ILEF and remarked that leprosy workers feel encouraged and proud through such relentless work by Ms. Watson in various leprosy-endemic countries.
Ms. Watson in her thankful reply was apreciative of the innovative work in prevention of disabilities by BLP and invited debate on controversial points on operational aspects of physical rehabilitation. She felt encouraged by the award conferred on her by the Gandhi Memorial Leprosy Foundation and observed that the struggle by leprosy workers the world over would continue until the disease is eliminated.
Dr. C. R. Revankar, Deputy Director of BLP, proposed a vote of thanks-Materials from R. Ganapati
National Seminar on Public Health Aspects of Fixed Duration Therapy in Leprosy. The proceedings of the Indian Association of Leprologists' (IAL) one-day seminar on the Public Health Aspects of Fixed Duration Therapy in Leprosy, held in Bombay on 22 September 1995, were received from Dr. C. R. Revankar, IAL Org. Secy., and are reproduced below:
"At the outset Dr. C. R. Revankar, Organizing Secretary, stated the purpose and objectives of holding the seminar. He said that keeping the mass scale program in mind, the seminar was expected to assess the validity of the present MDT for fixed duration in terms of treatment failure and relapses- their identification and frequency. In view of this, background papers were sought on i) laboratory aspects of fixed duration therapy, ii) clinico-bacteriological experience in FDT, iii) epidemiological aspects of FDT, iv) operational aspects of FDT, and v) operational aspects of FDT, national views.
Dr. M. D. Gupte, who chaired the proceedings, in his opening remarks stated that FDT had been already accepted for mass application and had already paid dividends by lowering the magnitude of the leprosy problem in the country, making the goal of elimination of leprosy attainable by 2000 A. D. However, he further mentioned, based on our present experience of FDT, that they had to find out if there were any areas which demanded special attention with respect to therapy. He hoped the papers and discussion would throw some light on that.
Dr. V. M. Katoch, in his paper on "Laboratory Aspects of FDT," presented the merits and demerits of various laboratory tools, i.e., MI, FDA-EB, Lamma, ATP, macrophage-based and various substrate uptake studies which could be considered to ascertain disease activity at the time of withdrawal of treatment, detect relapses and differentiate them from reversal reactions. He stressed that molecular biology techniques could be useful since several specific gene sequences of M. leprae had been identified. He, however, emphasized the use of PCR, based on RNA targeting assays. RNAbased methods were best for viability determination and BI plus RNA-PCR in smear-positive leprosy ribosomal RNA targeting assays had been found useful in confirmation of relapse, and also to differentiate between reaction and relapse.
He further pointed out that the present strategy of using corticosteroids to differentiate between relapse and reversal reaction was dangerous. He also replied to the questions and comments from the participants already sent to him. Dr. Katoch emphasized that there was no dispute on FDT. However, development of serological assays targeting antigen for live state may have a good future. Mr. S. S. Naik questioned whether PCR could be applied on a mass scale.
In the discussion following this paper. Dr. Poricha said that as far as histopathology of the lesion following FDT was concerned, even though granuloma persisted for a long time, the granuloma that laoked inflammation should be considered as one showing good response. Dr. Girdhar asked about the sensitivity of PCR techniques. Dr. Katoch said that sensitivity in untreated PB cases of DNA-PCR was 60% to 80% while that of RNA-PCR could reach 85%-90% or more, depending upon sampling and techniques employed.
Dr. P. Vijayakumaran, while presenting his paper on "Clinico-bacteriological Experience in FDT," stated that the initial BI had an influence on further bacteriological response. He presented data suggesting that the fall in BI was more pronounced during the first 2 years and it continued after RFT during surveillance. He also mentioned that a considerable number of patients had developed reactions during the first year of treatment and also during the surveillance period. There were, however, no data showing any correlation between reaction and bacterial clearance. He stated that in PB leprosy disease activity appears in the form of reactivation of old inactive lesion or persistence of active lesions or appearance of new lesions. Since this is not very clear, he felt there was need to set new criteria for identification of relapse in field conditions.
The paper on "Relapse following Fixed Duration Therapy for Multibacillary Leprosy" by Dr. S. K. Noordeen was read by Dr. Revankar. Only two cases of relapse occurred out of 6006 MB cases after 22, 397 person-years of follow up, from 6 trial centers like Bamako, Ccbu, China 1 and 2, Karigiri and Brazil.
Dr. R. Ganapati, while presenting his paper on "Operational Aspects of FDT," emphasized the need to train workers on FDT with the help of clinical photographs and diagrams envisaging newer concepts in therapy. He also pointed out the ambiguity in the reasoning for extending therapy beyond FDT in the program. He pointed out that there seems to be confusion among the workers with reference to stopping MDT. The chief reason probably was the lack of conviction on the part of workers to face the consequences.
Comments from the participants were exchanged after the presentation of background papers.
Dr. B. R. Chattcrjee showed bacteriological response in smear-positive cases in his study and expressed that withdrawal of DDS may possibly help in early clearance of bacillary debris.
Mr. Anand Iyer from the Foundation for Medical Research presented data on a secretory antigen. (Ag. 85 complex) and stated that this antigen was released, from growing bacteria and they could be estimated in patients sera using ELISA techniques. He felt this laboratory tool could be used to assess disease activity as the levels of this responded to therapy. However, the persistence of these antigenic signals after FDT/clinical subsidence pointed to limited usefulness of this approach for deciding activity/inactivity.
Dr. B. K. Girdhar showed data corelating a comparatively higher incidence of relapse in BL/LL patients with a high initial Bl. He mentioned that relapses due to drug-sensitive organisms following FDT in highly positive patients are not infrequent. It was opined that contary to the earlier belief that persister bacilli would disappear in their natural course, it may not be so.
Dr. P. S. Rao, while referring to Marchoux study said the relapses in patients with a high initial BI (i.e., 3+ or more than 3+) might occur even beyond years. He, therefore, suggested that all patients with an initial BI of more than 4+ might need treatment for more than 24 months. Dr. Rao also stated that the proportion of new-cases over recent years had almost remained the same. This indicated that transmission is going on.
Dr. J. A. Ponniah stated that there were many cases of relapse reported in certain areas. However, he pointed out that the initial BI, charting and identification of relapses were not satisfactory.
Dr. A. C. Parikh mentioned that PB patients posed major clinical problems as far as treatment was concerned, particularly when the size and number of the skin lesions increased. On this issue, Dr. Ganapati presented data on PB leprosy which showed the continued clinical regression of PB cases with 10 or more lesions who were treated with PB-MDT for months.
Dr. K. K. Koticha mentioned that careful measurement of the size of the lesion(s) periodically might help in showing clinical regression. He further emphasized the need to train field workers whenever there was a change in the strategy.
Dr. P. Krishnamurthy was of the opinion that the criteria of cure were not clear, particularly in cases with 3-9 lesions and especially with nerve lesion since these patients did not respond satisfactorily to 6 months of therapy.
Dr. K. Uday Kiran said the report showed that the relapse rate was very low after MDT of fixed duration and, thus, not likely to pose any public health problem.
Dr. T. H. Masood Ahmed showed the current data of Tamil Nadu on smear-positive MB patients and pointed out that very few of them had a BI of more than 4 + . He, however, insisted on giving these patients treatment for more than 2 years.
Dr. J. T. Kale presented the statistics for the state of Maharashtra, showing almost 10% patients were on extended therapy in 1994-95 since, according to doctors and nonmedical supervisors, the clinical response was not satisfactory. Through proper training, this proportion has been reduced to 1%.
Dr. V. K. Edward mentioned that relapses were mainly a clinical problem. Like any other disease, relapses in leprosy were bound to be expected and we should be prepared for them.
Dr. V. V. Pai, while making a brief clinical presentation on two smear-positive MB cases of BLP that had been closely followed up, wondered whether laboratory studies showing viable bacilli in these cases would be representing only persisters; however, (clinically) the patients have not relapsed over 5 years after FDT.
Mr. S. S. Naik remarked that patients with smear-positive leprosy were very important cases from a public health point of view. Therefore, there must be dross-notification of these patients whenever they moved from one place to another.
After thorough deliberations by the participants on various aspects of FDT, the following recommendations were formulated:
1. FDT has been accepted as a national policy under NLEP, due to its success in the field program with negligible relapse rate. However, relapses are encountered and these are found to be in the highly bacilliferous BL and LL group of MB patients with a BI of more than 4.0. Hence, it was recommended that MB patients with a BI of 3.0 and above should be studied as a separate group under research until further data on relapses are documented. Considering neuritic leprosy as MB for treatment purposes should be a matter for research.
2. Patients of the PB type with multiple skin and nerve trunk lesions pose special clinical problems in terms of persistent clinical activity and reversal reaction. For lack of authentic data on such an issue, it was difficult to draw a conclusion, although certain field data in small samples showed continued clinical regression even in the case of patients with multiple lesions treated with WHO-PB-MDT after stopping treatment. It was, therefore, recommended to consider this issue as a special area of research to enable further conclusions to be drawn.
3. Differentiation between reversal reaction and relapse clinically is considered to be difficult from the field point of view. Since laboratory support in terms of PCR is now available, it was recommended to use PCR based on RNA (mRNA/rRNA) targeting assays for viability studies to differentiate between reaction and relapse, wherever especially possible.
4. It was recommended that patients with smear-positive leprosy must be cross-notified whenever they migrate from one place to another.
5. To practice FDT in the field from public health and individual angles, appropriate training materials in the form of albums of color photographs, FDT folders, etc., should be developed to enable workers, dermatologists, and general medical practitioners to understand the subject as well as to help uncounselling patients.
Social Aspects of Leprosy (a classified bibliography, 1994) available. The Centre for Social Science Research on Leprosy, Gandhi Memorial Leprosy Foundation, Wardha 442 103, Maharashtra, India, has produced a document of 237 pages, with appendices, covering the whole subject of the social aspects in great detail. The project team for this remarkable, and probably unique, contribution included Dr. S. N. M. Kopparty (Senior Research Scientist), Dr.A. M. Kurup, Shri R. Giridhar and Shri K. Velayudham. The main subject headings cover epidemiology, leprosy control programs, survey education and treatment, compliance, deformities and disabilities, rehabilitation, knowledge and attitudes to leprosy, psychosocial aspects, social groups, genetics, leprosy organizations, health, leprosy and other diseases and research. The preparation of this bibliography was helped by contacts with the library of the Mahatma Gandhi Institute of Medical Sciences in Sevagram, the National Medical Library in New Delhi, the libraries of the Bombay Leprosy Project, the JJ Group of Hospitals in Bombay, the Jawaharlal Nehru Medical College and the Tropical Diseases Research Division of the World Health Organization. Enquiries to Dr. S. N. M. Kopparty as above (the document is heavy and it is likely that some contribution to postage costs may be needed)-Trop. Dis. Bull. 93 (1996) 333
Senegal. I LAD to hold Second Annual Doctor's Course in Practical Training on POD in Leprosy. The Second Doctor's Course in Practical Training on POD in Leprosy, organized by the Institut de Leprologie Appliquée de Dakar, will be held 9-19 December 1996. Information on the course, received from Dr. Michel-Yves Grauwin, follows:
Durée: 10 jours.
Nombre maximum de participants: 5
Dates: du 9 au 18 décembre 1996.
Objectifs: donner à des médecins des notions de base sur la lèpre et des concepts d'organisation pratique de tous les volets d'un PNL (PCT et PIRP) afin d'assurer une prise en charge globale des malades de la lèpre.
Langue: Français parlé couramment et e'erit. Niveau requis: Ce cours s'adresse aux Docteurs en Médecine et particulièrement aux responsables de PNL.
Contenu du cours: Pathogénie de l'infection lépreuse, concept PIRP, bacterio, diagnostic positif, formes cliniques et classification, neuropathies lépreuses, réactions, traitement, recueil des données, problèmes ophtalmologiques, atteintes fonctionnelles, bilan neuro, rééducation, soins aux MPP, éducation sanitaire, chirurgie et chaussures. Mode d'admission et conditions: Sur dossier, après analyse des objectifs professionnels et avec l'accord de prise en charge d'un bailleur de fonds couvrant les frais de voyage et de séjour.
Date limite de depot des candidatures: 1er Novembre 1996.
Cout: 150.000 francs CFA. Ce montant couvre les frais du cours, l'hébergement en chambre individuelle avec petit déjeuner et la fournitures des documents relatifs au cours. Ce montant ne comprend pas les frais de voyage aller et retour et les per diem. A verser à 1TLAD: compte bancaire nº 9520.770410.19-BICIS BP. 392- 2, avenue Roume, Dakar, Senegal; Télécopie: (221)23 37 07.
Pour tout renseignement, s'adresser au: Dr. I. Mane responsable de la formation, Docteur M. Y. Grauwin, Institut de Leprologie Appliquée de Dakar, BP. 11023, Dakar-CD, Sénégal; Télécopie: (221) 24.18.18.
Prevention of Disabilities and Rehabilitation in Leprosy course at ILAD. The 6th annual international course in Prevention of Disabilities and Rehabilitation in Leprosy, organized by the Institut de Leprologie Appliquée de Dakar in collaboration with DAHW-Senegal, will be held in 1997. We have received the following information from Dr. Michel-Yves Grauwin:
Dates: Module 1: 13 Février- 15 Mars 1997;
Module 2: 17 Mars-29 Mars 1997.
Nombre de participants: 8
Objectifs: Module 1: Former des responsables pour la mise en oeuvre, l'organisation et le développement des techniques de Réadaptation fonctionnelle, d'Education sanitaire et de Prévention des invalidités dans le cadre d'un Programme National de Lutte contre la lèpre.
Module 2: Formation à la rééducation préet post-opératoire des handicapés de la lèpreopérés.
Type d'enseignement: Participatif et pratique.
Contenu: Module 1 : Généralités sur la lèpre; prévention et prise en charge des atteintes nerveuses; chirurgie de la lèpre: indications; rescription et fabrication de chaussures adaptées; éducation sanitaire, conception, organisation, application et évaluation d'un Programme de Réadaptation; techniques de communication et formation des auxiliaires.
Module 2: Rééducation fonctionnelle d'une paralysie récente et des paralysies opérées. Amputation et appareillage.
Langue: Français parlé couramment et écrit.
Mode d'admission: Sur dossier, après analyse des objectifs professionnels.
Date limite de dépôt des candidatures: 15 Novembre 1996.
Condition d'admission: Ne seront retenus que les dossiers des candidats bénéficiaires d'une bourse couvrant les frais de voyage et de séjour.
Niveau requis: Kinésithérapeutes, ergothérapeutes et infirmiers-rééducateurs pour les modules 1 et 2; Infirmiers spécialistes-lèpre pour le module 1.
Pour tout renseignement, s'adresser au: Dr. J. L. Cartel, Directeur, Institut de Leprologie Appliquée de Dakar, BP 1 1023, Dakar-CD, Sénégal. Fax: (221) 24.18.18.
Switzerland. Dr. Lopez-Bravo retires. Dr. Luis Lopez-Bravo, Medical Officer with the Action Programme for the Elimination of Leprosy (LEP) at the World Health Organization, retired at the end of November 1995. His many friends in ILEP and throughout the world wish him a happy and active retirement. -ilep flash 5 (1995) p. 6
IMMYC and THEMYC meeting dates. The Steering Committee on Immunology of Mycobacterial Diseases (IMMYC) will meet in April 1997; deadline for proposals to this committee is February 1997. The Steering Committee on the Chemotherapy of Mycobacterial Diseases (THEMYC) tentatively set its meeting in February 1997; deadline for proposals for this committee is December 1996. -Information from TDR news 49 (1996) 7
Sasakawa Health prize awarded to Prof. Le Kinh Due and Dr. J. Torres Goita Torres. Prof. Le Kinh Due, Director of the Vict Nam National Control Programme, was awarded the Sasakawa Health prize by the World Health Organization in May 1995.
This prize is given to a person, institution or nongovernmental organization having accomplished outstanding innovative work in health development. This might include the promotion of given health programs or notable advances in primary health care in order to encourage the further development of such work.
The prize this year was also awarded to Dr. J Torres Goita Torres of Bolivia for his work in the delivery of general health care and active promotion of community participation.
Prof. Le Kinh Due has devoted nearly 40 years of his professional life to the campaign against leprosy in Viet Nam. In 1981 he established a comprehensive national leprosy eradication program. Since then, there has been a steady decrease of leprosy prevalence from 21 per 10,000 in the North and 31 per 10,000 in the South in 1959 to 1.6 per 10,000 in the whole country in 1993, while the proportion of new cases among children has decreased from 9% in 1959 to under 3% in 1991. Further, the disability rate among new cases dropped from over 34% in 1983 to under 18% in 1993, denoting a successful health education and control program.
Prof. Le Kinh Due contributed greatly to the elaboration of multidrug therapy (MDT) programs and their early application in Viet Nam. Owing to his sustained efforts and innovative strategies, Viet Nam has achieved the target of leprosy elimination according to WHO criteria in 205 out of the 527 districts in Viet Nam, covering 50.6% of the total population.-ilep flash 5 (1995)
U.S.A. Parkers honored for service to those with leprosy. The Massachusetts Department of Public Health unveiled a commemorative plaque in honor of Frank H. Parker, M. D., who served as Superintendent of Penikese Hospital, Buzzards Bay, from 1907-1921 and his wife, Marian, for their dedicated service to those with leprosy on Monday, 8 April 1996 in the Nurses Hall of the State House in Boston.