- Volume 64 , Number 3
- Page: 274–81
Comparative trial of steroids and surgical intervention in the management of ulnar neuritis
ABSTRACT
Fifty-seven ulnar nerves in 39 patients with early neuritis were studied to assess the benefits offered by medial epicondylectomy and external decompression in addition to steroid therapy. The patients were randomly allocated to the surgical or medical group. In those cases where there was bilateral involvement, surgery was carried out on only one side. All cases were assessed prior to treatment and after the first and second years following treatment. The improvement in motor and sensory functions attained at the end of the first year was sustained into the second year. The improvement sustained in both groups was similar even in the second year, and medial epicondylectomy with external decompression seems to have no added benefit as compared to steroid therapy alone in the early treatment of ulnar neuritis. Early diagnosis and treatment, especially in borderline lepromatous cases, seem to offer some hope of nerve function recovery.RÉSUMÉ
Cinquante-sept nerfs cubitaux de 39 patients avec une névrite précoce ont été étudiés pour évaluer les bénéfices offerts par une épicondylectomie médiane et une décompression externe en plus du traitement par stéroïdes. Les patients ont été répartis au hasard entre le groupe chirurgical et le groupe médical. Dans les cas où il y avait une atteinte bilatérale, la chirurgie n'a été réalisée que d'un seul côté. Tous les cas ont été évalués avant le traitement, et après la première et al deuxième année après le traitement. L'amélioration des fonctions motrice et sensorielle obtenue à la lin de la première année a été conservée dans la deuxième année. L'amélioration obtenue dans les deux groupes était semblable même dans la deuxième année, et l'épicondylectomie médiane avec décompression externe ne semble pas avoir apporté de bénéfices supplémentaires, comparée au traitement pare stéroïdes seuls dans le traitement précoce de la névrite cubitale. Le diagnostic précoce et le traitement, particulièrement dans les cas borderline lépromateux, semble offrir quel qu'espoir de récupération de la fonction nerveuse.RESUMEN
Se estudiaron 57 nervios ulnares en 39 pacientes con neuritis temprana para comparar el beneficio derivado de la epicondilectoniía medial y la descompresión externa con el derivado de la terapia con esferoides. Los pacientes fueron repartidos al a/ar en el grupo quirúrgico o en el grupo médico. En aquellos casos donde hubo afección bilateral la cirugía se practicó sólo en uno de los lados. Todos los casos fueron valorados antes del tratamiento y después del primer y segundo años de tratamiento. La mejoría en las funciones sensorial y motora lograda al final del primer año se sostuvo en el segundo año y fue similar en ambos grupos. La epicondilectoniía medial con descompresión externa no parece tener efectos benéficos adicionales a los que se logran con la terapia con esferoides. El diagnóstico y el tratamiento temprano, especialmente en los casos de lepra lepromatosa, aumentan las posibilidades de recuperación de la función nerviosa.Early detection and adequate treatment of neural impairment is important in the primary prevention of disabilities in leprosy (10). Steroid therapy together with continuation of antileprosy drugs is generally accepted as the treatment of choice in acute neuritis (6). On the other hand, the role of surgical decompression in the treatment of neuritis has been mainly to relieve pain. However, some of the studies also showed improvement in both motor and sensory functions (1,4,7,8). It is not very clear whether a combination of surgical decompression and steroid therapy would be more beneficial.
Steroid therapy alone and in combination with surgical decompression was tried in the treatment of ulnar neuritis in a study done at the Schieffelin Leprosy Research and Training Centre, Karigiri, India, between 1980 and 1982. The results at the end of the first year indicated that there was no added benefit in carrying out external decompression in cases of early ulnar neuritis being treated with steroids (5).
Since some nerves continued to change in their function even after I year, the second year results were evaluated to see if the first year improvement was lasting, and if there was any added benefit for the surgical decompression over a longer period. The opportunity was used to study the influence of factors such as disease classification, duration of neuritis and severity of neuritis on recovery of nerve impairment, which were not discussed in the earlier paper (5).
MATERIALS AND METHODS
The modalities of treatment were named: 1) treatment with steroids (Medical group) and 2) steroids combined with medial epicondylectomy and external decompression (Surgical group). The intake of patients and methodology have been described earlier (5).
Patients were allotted randomly to the two groups. In patients with bilateral involvement, the right side was allocated to the group drawn by random selection while the left side was treated as the other group. After the initial assessment of nerve function, treatment was started. After completion of treatment, the patients were followed up at the end of 1 year and again at the end of 2 years.
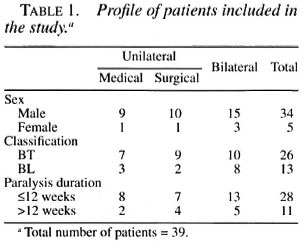
Fifty-seven patients with involvement of 75 ulnar nerves were included in the study (18 bilateral cases). Eighteen patients were lost to follow up, so at the follow up after 2 years there were 39 patients with 57 nerves (18 bilateral cases). The Medical group had 28 nerves and the Surgical group, 29 nerves. The Medical and Surgical groups' profiles are shown in Table 1.
The methods of treatment were evaluated by assessing the nerve function in terms of motor and sensory recovery. Nerve function was assessed by the Voluntary Muscle Test (VMT) and a sensory test (3). The VMT involved grading of the abductor digiti minimi, first dorsal interosseous and the third palmar interosseous using the Medical Research Council Grading. The sum of the grades of these three muscles was expressed as the voluntary motor score. The maximum VMT score was 15.
Sensory testing was done at 15 predetermined sites over the ulnar nerve distribution, and the total number of sensitive points was expressed as the Sensory score. Sensation was tested using No. 3 Nylon (0.38 in diameter). One point was given for each correct response to No. 3 Nylon, making a maximum score of 15. No. 6 Nylon (0.75 mm in diameter) was used only on those sites which showed misreference or showed no response to No. 3 Nylon. Half a point was given for each correct response to No. 6 Nylon.
The predetermined sites for sensory testing were: 1) on the volar aspect of the little finger, two points each over the ulnar border of each phalanx and two points on the ulnar border of the palm were tested for a total of eight sites on the volar surface. 2) on the dorsal aspect of the little finger, one point on the distal phalanx, two points each on the middle and proximal phalanges, and two points on the ulnar border of the dorsum of the hand were tested for a total of seven sites on the dorsum.
Motor and sensory scores graded as"good," "moderate," "bad" and "absent orparalyzed" are shown in Table 2.

Impairment of less than 3 months' dura-tion was classified as "recent," if longerthan 3 months, as "old." The Wilcoxon signed rank test was used to compare thescores of the second year with those of ad-mission and of the first year. For testing thesignificance of improvement between theMedical and the Surgical groups, the Mann-Whitney U test was used.
RESULTS
VMT score. The average improvement in the VMT score from the time of admission to the end of the second year was very similar to the improvement at the end of the first year, indicating sustenance of the improvement of motor function. This was statistically significant for both the Medical (p < 0.05) and the Surgical (p < 0.01) groups. However, the improvement in motor function from the first year to the second year was not statistically significant in either group (Table 3).
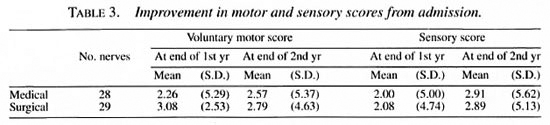
Sensory score. The average improvement in the Sensory score from the time of admission to the end of the second year was similar to the improvement at the end of the first year, indicating sustenance of improvement in sensory function, and was statistically significant for both the Medical (p < 0.05) and the Surgical (p < 0.01) groups. The improvement in sensory function from the first year to the second year was not statistically significant in the Surgical group, but was significant in the Medical group (p < 0.05) (Table 3).
Medical and Surgical groups. There was no significant difference in the improvement between the Medical and Surgical groups for both VMT and Sensory scores at the end of the second year (Table 3).
Nerve tenderness. Nerve pain and tenderness cleared completely at the end of the first year in both groups, and none of the patients had nerve pain or tenderness at the end of the second year.
Type of leprosy. The improvement in the VMT score when comparing borderline tuberculoid (BT) and borderline lepromatous (BL) groups was not statistically significant. However, the improvement in Sensory scores for the BL group was better than the BT group, and it was statistically significant (p < 0.01) (Table 4).
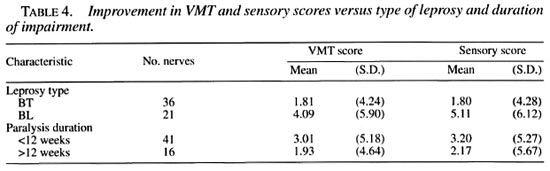
Recent versus old impairment. Patients with recent impairment showed better improvement compared to patients with old impairment (Table 4), but this was not statistically significant.
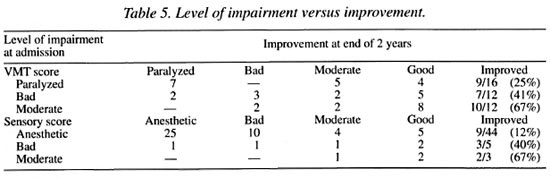
Level of impairment. The level of impairment at the beginning of treatment had an influence on the outcome. Only 25% of patients with motor paralysis and 12% with complete anesthesia improved to good function at 2 years compared to 67% for patients with moderate impairment (Table 5).
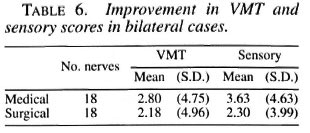
Bilateral cases. Eighteen bilateral cases provided an opportunity to compare both treatment modalities under the same conditions. Both the Medical and Surgical treatment modalities have shown similar improvement. Nerve damage in bilateral cases tends to be symmetrical on both sides (Table 6).
DISCUSSION
The individual VMT score reflects only the sum improvement of the three muscles and does not assess improvement in the individual muscle. Assessment of improvement in the individual muscle would be more appropriate since this can be correlated to function. Grading small muscles of the hand from grades 0 to 2, using the Medical Research Council Scale, is extremely difficult and is not easily reproduced. The improvement from grade 0 to grades 1 or 2 also does not have any functional significance. It would be more appropriate to consider only improvement to grade 3 or above as significant.
The VMT and Sensory scores at the end of the second year indicate that the first year improvement was lasting into the second year, and there was no added benefit for the external decompression group even over a longer period. Even though some cases continued their improvement into the second year the improvement was not significant.
The tendency of BL cases to show better improvement in sensory scores compared to the BT cases is seen in this study as in other studies (2,9). An explanation for this is not readily found but a lesser degree of immunological damage in the BL cases could be understood as a possibility. However, the improvement in VMT scores for BL cases over BT cases in this study was not significant.
The results in relation to the duration of paralysis seem to suggest that patients diagnosed and treated within 3 months of onset of neuritis seem to have a better chance for recovery (although statistically not significant) than patients who are diagnosed and treated after 3 months. Since the level of impairment had a significant effect on the outcome, earlier detection of nerve function impairment using more sensitive nerve assessment methods assumes great importance.
The role of medial epicondylectomy as a decompressive procedure is limited since it relieves only extraneural pressure. Procedures such as hemicircumferential epineurotomy and interfascicular neurolysis, which relieve both intraneural and extra-neural pressures, need to be evaluated to see if they offer any additional benefit over steroid treatment.
REFERENCES
1. Enna, C. D. and Jacobson, R. R. A clinical assessment of neurolysis for leprous involvement of the ulnar nerve. Int. J. Lepr. 42(1974)162-164.
2. Kikan, K. U., Stanley, J. N. A. and Pearson, J. M. H. The outpatient treatment of nerve damage in patients with borderline leprosy using semistandardised steroid regimen. Lepr. Rev. 56(1985 )127-134.
3. Lewis, S. Reproducibility of sensory testing and voluntary muscle testing in evaluating the treatment of acute neuritis in leprosy patients. Lepr. Rev. 54(1983)23-30.
4. Oommen, P. K. Ulnar nerve decompression by medial epicondylectomy of the hunerus and a method of assessing muscle power status by totalling the muscle grading. Lepr. India 51(179)336-340.
5. Pannikar, V. K., Ramprasad, S., Rosi Reddy, N., Andrews, P., Ravi, K. and Fritschi, E. P. Effect of epicondylectomy in early ulnar neuritis treated with steroids. Int. J. Lepr. 52(1984)501-505.
6. Pearson, J. M. The use of corticosteroids in leprosy. Lepr. Rev. 52(1981)293-298.
7. Said, G. Z., Zodhy, A. and El-Akkad, I. N. External and internal neurolysis of ulnar and median nerves in leprous neuritis. Lepr. Rev. 44(1973 )36-43.
8. Thomas, A. A., Selvapandian, A. J., Alexander, R., Sam, S., Joseph, D. and Chellan, P. P. A comparative study of surgical decompression by medial epicondylectomy and medical decompression by steroids for the management of ulnar neuritis and early paralysis. Lepr. India 51(1979)599-600.
9. Touw-Langendijk, E. M. J., Brandsma, J. W. and Anderson, J. G. Treatment of ulnar and median nerve function loss in borderline leprosy. Lepr. Rev. 55(1984)41-46.
10. Watson, J. M. Essential action to minimise disability in leprosy patients. London: The Leprosy Mission International, 1988.
1. M.S. (Orthopedics), Associate Surgeon.
2. Coordinator.
3. M.S. (Orthopedics), Head, Branch of Surgery, Schieffelin Leprosy Research and Training Center, Karigiri 632 106, North Arcot District, Tamil Nadu, India.
Received lor publication on 15 May 1995.
Accepted for publication in revised form on 25 January 1996.