- Volume 63 , Number 4
- Page: 507–17
Prevention of impairment in leprosy; results from a collaborative project in China
ABSTRACT
Objective-to evaluate programs of prevention and treatment of impairments due to leprosy in 8 geographical areas in the People's Republic of China. Design-follow up of cohorts of leprosy patients receiving a range of different interventions. Setting-8 different geographical areas in China, varying in urban and rural characteristics f rom 6 provinces and 2 municipalities. Subjects-leprosy patients who were receiving or had completed a course of antileprosy chemotherapy. Interventions-a range of interventions, including steroids, self-care training, adapted footwear, surgery and provision of prothèses. Main outcome measures-changes in eye, hand and foot impairments between baseline assessment and assessment at 2 years. Results-232 out of 3571 patients assessed monthly over 2 years developed acute neuritis and, in most areas, were promptly and adequately treated. Regular self care of eyes was established in 238 out of 313 patients with lagophthalmos and was associated with reduction in the prevalence of conjunctivitis. Regular self care of hands was established in 730 out of 1010 patients with neurological impairment of the hand; this was associated with a reduction (80%) in hand cracks and wounds. Regular self care of feet was established in 745 out of 1094 patients with neurological impairment of the feet; this was associated with a 83% reduction in patients with cracks and a 33% reduction in patients with sole wounds. A footwear program was established in all 8 areas providing footwear to 4698 patients over the 2-year period; this was associated with a reduction of 61% and 21% in patients with cracks and wounds, respectively. Management of complicated sole wounds in 256 patients resulted in 69% of these patients being free of sole wounds at 2 years. Targets for reconstructive surgery and amputations were not fully attained, but lower limb prostheses were provided for 306 patients. Conclusions-leprosy is a chronic disease characterized by peripheral neuropathies which can result in increasing secondary impairments and disabilities. The emphasis, in countries such as China where the chemotherapy programs have been effectively implemented, is shifting to prevention and treatment of impairments. This innovative program in China has successfully demonstrated that it is possible to prevent and reverse impairments due to leprosy.RÉSUMÉ
Objectif-évaluer des programmes de prévention et de traitement de dommages dûs à la lèpre dans huit zones géographiques de la République Populaire de Chine. Méthode-suivi de cohortes de malades de la lèpre recevant une variété d'interventions. Localisation-huit zones géographiques différentes de la Chine, différant quant à leurs caractéristiques urbaines et rurales, provenant de 6 provinces et deux municipalités. Sujets-des malades de la lèpre qui recevaient ou avaient terminé une chimiothérapie anti-lépreuse. Interventions-diverses, y compris des stéroïdes, une formation aux soins personnels, des chaussures adaptées, la chiurgie et une série de prothèses. Principales mesures d'impact-changements dans les dommages oculaires, des mains et des pieds, entre l'évaluation initiale et l'évaluation après deux ans. Résultats-232 des 3571 malades évalués mensuellement an cours des deux ans ont développé une névrite aiguë, et, dans la plupart des régions, ont été traités rapidement et adéquatement. Les soins personnels réguliers des yeux ont été mis en route chez 238 des 313 patients ayant un lagophtalmos, et ont été associés à une réduction de la prévalence des conjonctivites. Les soins personnels réguliers des mains ont été mis en route pour 730 des 1010 malades présentant des dommages neurologiques de la main; ceci a été associé à une diminution (80%) des crevasses et des blessures des mains. Les soins personnels réguliers des pieds ont été mis en route chez 745 des 1094 malades avec des dommages neurologiques des pieds; ceci a été associé à une diminution de 83% des malades avec des crevasses et une diminution de 33% des malades avec des blessures plantaires. Un programme de chaussures a été mis en place dans toutes les huit régions, fournissant des chaussures à 4698 malades au cours de la période de deux ans; ceci a été associé à une réduction des crevasses et des blessures plantaires de respectivement 61% et 21%. La prise en charge de blessures plantaires compliquées chez 256 malades fit que 69% de ces maladcs n'avaient plus de blessures plantaires après deux ans. Les objectifs pour la chirurgie reconstructrice et les amputations n'ont pas été entièrement atteints, mais des prothèses de membre inférieur ont été fournies à 306 malades. Conclusions-la lèpre est une maladie chronique caractérisée par des neuropathies périphériques qui peuvent avoir pour conséquence une augmentation des dommages secondaires et des incapacités. Dans des pays comme la Chine où les programmes de chimiothérapie ont été effectivement réalisés, on met progressivement l'accent sur la prévention et le traitement des incapacités. Ce programme novateur en Chine a démontré avec succès qu'il est possible de prévenir et de réparer les dommages causés par la lèpre.RESUMEN
Objetivo: evaluar los programas de prevención y de tratamiento de las secuelas de la lepra en 8 áreas geográficas de la República Popular China. Diseño: seguimiento de cohortes de pacientes con lepra sujetos a diversas intervenciones. Localidades: ocho diferentes áreas geográficas de 6 provincias y 2 municipalidades de China, con características rurales o urbanas. Individuos: pacientes con lepra en tratamiento o pacientes que hubieron completado un esquema de tratamiento con poliquimioterapia. Intervenciones: tratamientos con cstcroidcs, entrenamiento para su autoayuda, adaptación de calzado, cirugía y provisión de prótesis.Principales mediciones: cambios oculares y afección de manos y pies al momento de iniciar el estudio y dos años después. Resultados: Doscientos treinta y dos de 3571 pacientes revisados mensualmente durante 2 años, desarrollaron neuritis aguda. En la mayoría de las áreas, estos pacientes fueron pronta y adecuadamente tratados. En 238 de 313 pacientes con lagoftalmos se instituyó el cuidado personal y regular de los ojos dando como resultado una reducción en la prevalência de conjuntivitis. El cuidado personal de las manos instituido en 730 de 1010 pacientes con algún tipo de daño neurológico, dio como resultado una reducción del 80% en las cuarteaduras y lesiones de las manos. El cuidado personal y regular del pie establecido en 745 de 1094 pacientes con alteraciones neurológicas, condujo a una reducción del 83% en la frecuencia de cuarteaduras y a una reducción del 33% en la frecuencia de lesiones plantares. En el periodo de 2 años que duró el estudio, se proporcionó calzado a 4698 pacientes de las 8 áreas geográficas; esto estuvo asociado con una reducción del 61% y 21% en el número de pacientes con cuarteaduras y lesiones, respectivamente. El tratamiento de las lesiones plantares complicadas en 256 pacientes, condujo a la curación total del 69% de los pacientes en el periodo de 2 años. Así mismo, se proporcionaron prótesis para miembros inferiores a 306 pacientes. Conclusiones: la lepra es una enfermedad crónica caracterizada por neuropatías periféricas que pueden dar como resultado un aumento en las alteraciones incapacitantes secundarias. En países como China donde los programas de tratamiento con poliquimiotcrapia están bien establecidos, se hace énfasis en la prevención y tratamiento de las lesiones incapacitantes. Este innovativo programa ha demostrado que es posible prevenir y revertir las incapacidades debidas a la lepra.
Leprosy is a chronic, disabling disease caused by Mycobacterium leprae which principally affects the skin and peripheral nerves. The disease process also affects other organs, but it is the damage to peripheral nerves which is responsible for the impairment associated with leprosy. The primary damage to peripheral nerves causes loss of sensory, motor and autonomic function; these changes predispose toward secondary damage through trauma, abnormal pressures and secondary tissue infection leading to tissue damage and tissue loss. The process, once the primary nerve damage has occurred, is progressive, leading to increased impairment and disability (5).
The priority of the World Health Organization (6), nongovernmental organisations (8) such as ILEP (International Federation of Anti-Leprosy Associations), and most national leprosy programs has rightly been to prevent the primary nerve damage by early diagnosis and effective treatment of leprosy using multidrug therapy (MDT). The global leprosy program is increasing its coverage (11) rapidly, as seen in many countries, and the People's Republic of China is a good example. Acute nerve damage can occur during the course of antileprosy treatment using MDT, either silently or in association with acute changes in the skin (reversal reactions). This acute nerve damage can be reversed by treatment with corticosteroids, provided the nerve function changes are detected early and treated promptly. The most effective way of detecting and treating acute nerve damage in leprosy is currently under investigation in a number of centers. It is important that leprosy control programs effectively detect and treat acute nerve damage as well as provide antileprosy chemotherapy (3).
Once permanent damage has occurred to peripheral nerves the outcome is usually one of increasing impairment. The process in the hands and feet is of recurrent trauma, ulceration, tissue infection and, finally, permanent tissue loss including bone sequestration and, in some cases, amputation. The process following facial nerve paralysis is of recurrent conjunctivitis, exposure keratitis, and eventual blindness. Many leprosy programs include measures to prevent disability, and there have now been published recommendations for such programs (2-9). Some consider such disability prevention programs to be expensive and ineffective, although well intentioned. In this collaborative study we have attempted to address the question of whether or not a program of disability prevention can prevent or reverse impairment in leprosy.
The collaborative project was set up in 1989 jointly by the Ministry of Public Health of the People's Republic of China and The Leprosy Mission International. The project was to be a pilot for a national program and included eight different geographical areas in China. The project was run between 1990 and 1992 and evaluated by a joint team which included independent experts. The MDT program in China has been effectively implemented (12) so that the prevalence of leprosy patients requiring chemotherapy is now very low (0.17 per 10,000) and the incidence of new cases is very low (0.32 per 100,000). However, there remain substantial numbers of patients with permanent nerve damage who have completed chemotherapy, estimated at 200,000 at the time of the pilot project. Details of the impairments and disabilities caused by leprosy in China have been studied (13), suggesting that disability rates in China are high. China is, therefore, an appropriate country in which to conduct this study since there are high levels of disability associated with leprosy and disability is given a high priority following the effective implementation of MDT. The leprosy care in China is implemented by a well-staffed vertical program. The findings are important to the planning of a national approach to disability prevention and rehabilitation in leprosy in China, and also to many other countries planning to implement similar disability prevention programs.
MATERIALS AND METHODS
The study was coordinated by the Institute of Dermatology of the China Academy of Medical Sciences (CAMS) based in Nanjing and was jointly funded by the Ministry of Public Health (MOPH), Beijing and by The Leprosy Mission International (TLMI), London.
Study population
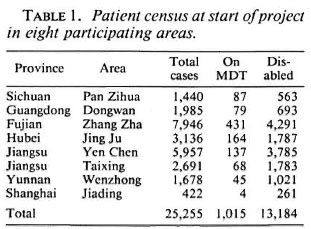
Eight different project areas were selected in six different provinces (Sichuan, Guangdong, Fujian, Hubei, Jiangsu, and Yunnan); these represented a range of urban (Shanghai and Taixing) and rural situations as well as different parts of China with substantial numbers of leprosy patients. A total census of all living leprosy patients in the pilot areas was completed prior to the commencement of the program of prevention; the findings are shown in Table 1. This census included patients on chemotherapy, those under surveillance, and all living patients who had completed chemotherapy. The definition of disabled included all patients found to have any impairment of nerve function, including those with sensory loss only.
Prevention program and evaluation
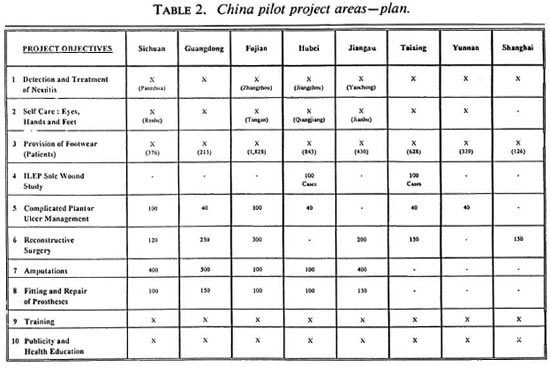
The prevention program was coordinated from CAMS in Nanjing where the protocols for nerve function assessment were standardized and the staff and patient training programs planned. The program was divided into 10 separate parts with different patient groups selected for each aspect. Some parts of the prevention program were common to all areas; this included detection and treatment of neuritis, self care, provision of footwear, training, publicity and health education. Some aspects, such as surgery, amputations, prostheses provision, and the sole wound study, were not carried out in every area. The details of which aspects were performed in which areas and the target numbcr of cases are presented in Table 2. A detailed description of the intervention program and its objectives and evaluation criteria is presented in the Appendix.
The evaluation procedures were planned at the outset along with the program protocol. The evaluation at the end of the 2-year project period was undertaken by a joint team of 55 investigators representing the China Academy of Medical Sciences, the Ministry of Public Health, the individual project staff, The Leprosy Mission International as well as independent experts. The final evaluation took place over 3 weeks with site visits to all areas. Central to the evaluation and to the program itself was the assessment and recording of impairments. This required the development of a specific form to record impairments and sequential changes in impairments over time, and the training of staff to perform and record impairments using the form (10). Sensation was tested with a ball-point pen and recorded at10 sites on the palmar surface of each hand and at 12 sites on the plantar surface of each foot. Wounds and cracks were observed and recorded graphically. Bone loss was recorded at the sites where sensation would have been tested. Lid gap was measured and recorded in millimeters and muscle strength was assessed and recorded on a 3-point scale of normal, weak and paralyzed.
RESULTS
The results of the pilot projects are presented by pilot area and by program aspect. The findings are shown as either the status at the end of the 2-year period or the change from baseline to the end of the 2-year project period.
Detection and treatment of neuritis
A total of 3571 patients in the eight pilot areas were followed up by monthly nerve function assessment to detect neuritis. During the study period, 232 (6.5%) of the group were diagnosed as having neuritis; 148 of these were classified as acute neuritis with accompanying pain and signs of reaction. The neuritis rates ranged from 1.7% in Jiangsu (Yen Chen) to 17.9% in Shanghai (Fig. 1); the rate also varied from 24.6% in newly diagnosed cases to 4.9% in those under surveillance after completing MDT. The differences between areas was largely explained by variations in the proportion of newly diagnosed patients being followed up in each area. In 7 out of the 8 pilot areas neuritis was treated promptly (within 1 month of diagnosis) but considerable delays were identified in one area. Patient compliance with steroid therapy was good but in some patients the degree of recovery was minimal.
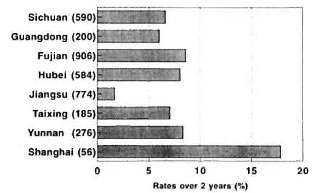
Fig. 1. Rates of neuritis in each project area. Figures in parentheses are number of cases followed up; = rates (%).
= rates (%).
Self care of eyes, hands, and feet Eyes. At the end of the 2-year period a good level of regular eye self care was achieved in 238 out of the 313 patients with lagophthalmos; there was reduction in conjunctivitis in 6 areas, no change in 1 area and a slight increase in 1 area. The area which failed to achieve regular self care in a high proportion of patients showed a reduction in conjunctivitis. The increase in conjunctivitis in Taixing was small and could have been explained by seasonal variation. The findings are shown in Figure 2.
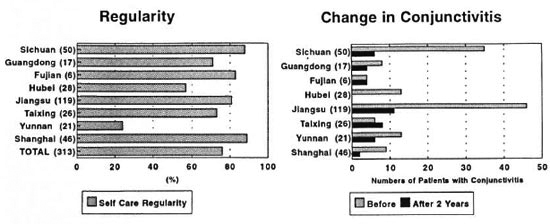
Fig. 2. Self care of eyes: regularity and change in conjunctivitis. Figures in parentheses are number of casesfollowed up.
Hands. A total of 1010 patients were enrolled in this aspect, and 102 of these patients had strength loss without sensory loss. At the end of 2 years, 72% (730) had achieved regular habits of self care; in two areas, however, this was less than 50%. There was an 80% reduction in patients with skin cracks (120 to 24) and patients with hand wounds fell from 12 to 1. The number of patients with bone loss increased from 162 to 167. A summary of the findings is shown in Figure 3.
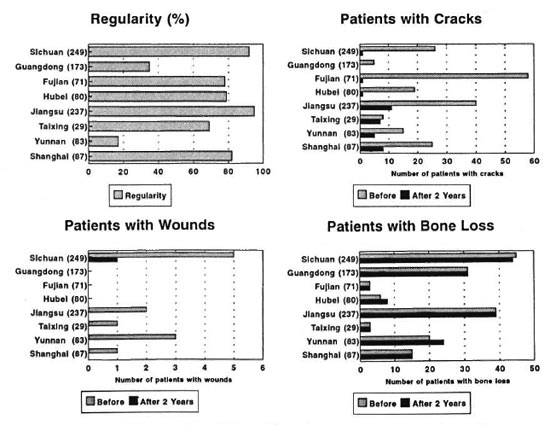
Fig. 3. Self care of hands; regularity and changes. Figures in parentheses are number of cases followed up.
Feet. A total of 1094 patients participated in the foot self-care aspect of the program and were followed up for 2 years. At the end of 2 years 68% (745) were judged to be regular in self care but in two areas, the same areas which performed poorly in hand self care, the regularity was below 50%. The numbers of patients with cracks reduced from 182 to 31 (83%) and those with wounds from 270 to 182 (33%). There was an actual reduction of 86% in the number of cracks and 35% in the number of wounds. There was an increase in the number of patients with bone loss from 264 to 267. The findings are shown in Figure 4.
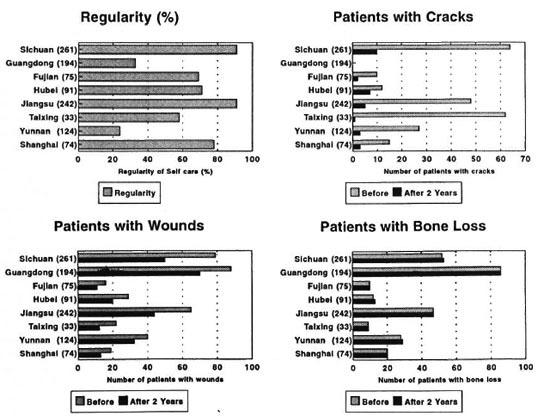
Fig. 4. Self care of feet; regularity and changes. Figures in parentheses are number of cases followed up.
Regularity in self care for eyes, hands and feet was seen to increase over the first year and to plateau after 1 year. Regular performance did not occur immediately after the first training session but required three monthly reinforcements to achieve reasonable levels of performance. A trend of increasing reduction in cracks and wounds in hands and feet was associated with increasing regularity of self care across the eight project areas.
Footwear program
In all project areas footwear was to be provided to patients with insensitive feet. A total of 4698 patients received 16,536 pairs of footwear over the 2-year period. Each project area worked on finding locally acceptable and locally available appropriate footwear. The cost per pair varied from US$4 to US$8 per pair and durability ranged from 2 to 6 months, depending on the type of footwear and the usage. Most pilot projects identified suitable footwear which varied in style between urban and rural areas. Some had tried Velcro fastening but had not found this satisfactory since it wore out quickly. Patients were recruited into the pilot projects over the 2-year period and so only 3109 patients had baseline and followup examinations. In this group the number with cracks was reduced from 301 to 118 (61%), with the actual number of cracks being reduced from 515 to 213 (59%). The number of patients with wounds was reduced from 1089 to 857 (21%), and the actual number of wounds was reduced from 1428 to 1160 (19%). Patients followed up for 2 years showed a greater reduction in wounds (44%) compared with those followed up for only 1 year (16%). Few areas succeeded in providing specialized shoes, such as shoes with moulded insoles.
ILEP sole wound study
This 3-year multicenter study included two centers in China-Taixing and Hubei. Hubei recruited 100 patients who met the study criteria; Taixing recruited 86. Both study centers lost five patients through migration or death, and in Taixing a further 15 had incomplete annual follow ups. The number of patients with wounds was reduced by 78% in Hubei and by 31% in Taixing. The actual number of wounds reduced by 82% and 10%, respectively. The conduct of the two centers had been different and the outcomes were different also. The Taixing center voluntarily decided to continue the study for another year to try to replicate the Hubei findings.
Management of complicated plantar ulcers
A total of 256 patients with complicated plantar ulcers were recruited in six pilot areas with successful treatment in 176 (69%) assessed by healing of the complicated ulcer. However, 42 had relapsed before the end of the 2-year follow up. Management varied greatly between the areas, including rest, surgery, dressings, self care, and use of plaster of Paris. The centers which undertook surgical excision of necrotic tissue after radiological examination of the affected feet had better success rates.
Reconstructive surgery
The number of surgical procedures carried out was 467, considerably less than the target of 1170, due to the lack of suitable patients in some areas and the lack of expertise in other areas. The procedures performed were 183 lagophthalmos corrections, 132 foot drop corrections, 71 eyebrow transplants, 31 facial paralysis repairs, 23 claw hand procedures, and 11 thumb opposition operations. Few areas had undertaken detailed postoperative measurements so that evaluation was largely subjective.
Amputations
Few new amputations were performed due to improved self care and better management of complicated ulcers.
Prosthesis
A total of 332 prostheses were fitted to 306 patients, the majority were below the knee but 37 were above-knee prostheses. Some areas used plastic prostheses; in other areas aluminum was used. In some areas a dedicated facility for leprosy patients was used while in others general rehabilitation facilities were utilized. Most patients reviewed had satisfactory prostheses and very few had stump ulcers.
Staff and patient training
Simple questionnaires were used to test the knowledge of staff and patients, and assessment of practical skills was performed by members of the visiting evaluation teams. The level of knowledge and performance in all areas was uniformly high.
Patient education
Each area produced their own training and education materials, and there was some exchange of ideas between areas as part of the overall project. The general quality and availability of the materials was good. Some material tended to have too much text, and booklets and posters which had the word leprosy in the title were found to be unpopular with patients.
DISCUSSION
This program was a series of pilot projects testing 10 different interventions in disability prevention in eight differing geographical areas. The program formed a pilot project prior to the implementation of a national program of disability prevention and, as such, proved an important learning experience not just for China but also for other countries where disability due to leprosy remains a significant problem. The program was, in general, very well run and most planned tasks were completed. However, some targets were not fulfilled such as the provision of moulded footwear, surgery and amputations. There was no control area in this study where impairments were monitored without any interventions. However, it was possible to compare the outcome between the different areas. The secular trend in impairments and disability due to leprosy reported by previous studies, as historical controls (7), has been of increasing disability so that the sustained improvements after 2 years which have been demonstrated in this study in China can be considered significant.
The frequency of neuritis in this study over the 2-year period is related to the classification and timing of MDT treatment as has been observed in other studies (1). The case mix of these factors largely accounts for the apparent geographical variations. The priority groups in the monitoring of nerve function for acute change are the newly diagnosed and those on MDT; the value of monitoring patients decreases with time after completion of MDT. The steroid regimen was, in general, used promptly and compliance was good. In one area there were significant delays in starting treatment due to issues concerning who was permitted to authorize treatment. This has now been changed.
Regular self care of the eyes, hands and feet was achieved in 6 out of the 8 pilot areas. In these pilot projects the eyes, hands and feet tended to be treated separately. However, it is recommended for the national program that this is done in a more integrated way. It is worth noting that regular self care was not achieved instantly and really developed over the 2-year period by repeated teaching; self care is a life-long habit which cannot be developed quickly. The two areas where self care was not well achieved were probably the most and the least developed areas, and the underlying explanations were likely to be very different. New approaches are needed in these areas, and it is important to recognize for the national program that while standard approaches may work in general there will be areas in which different methods, such as more community involvement or group sessions, will be needed to achieve regular self care behavior patterns. However, it is noted from the results that improvements in cracks and wounds do occur when self care is less than regular, and that improvements tend to be greater in areas with higher rates of self-care performance.
Footwear programs were effectively established in all areas but using different shoes. The issue of acceptability to patients seemed very important, and the types of shoes found to be acceptable varied among the pilot areas. The cost per year needs to be considered in comparing shoes of differing cost and durability. The shoes used lasted around 6 months on the average, shorter than is experienced elsewhere, which may reflect greater usage and the use of shoes in rough mountainous terrain. In some areas, patients wanted to buy their own shoes and needed advice on appropriate footwear.
The management of complicated ulcers was particularly successful as indicated by the numbers of patients who were ulcer free at the end of 2 years. Adequate surgical treatment, including debridment, sequestrectomy and excision of metatarsal heads, was important to long-term success. The reduced number of amputations conducted was a good indication of improved management of wounds and self care generally. Success with prostheses required regular follow up and repairs where needed; simply a supply of prostheses was not adequate.
The training of staff and patients was perhaps the largest part of the whole program and the secret of its success. The need for new approaches to the prevention of disabilities has been recognized (4). This study has clearly shown that prevention and reversal of impairments due to leprosy is possible-an extremely important finding. Regular self-care behavior takes time to become established, and this study shows the importance of regular reinforcement of training. Many have become disillusioned with attempts at preventing disabilities (McDougall, A. C. The prevention and management of disability in Hansen's disease control programs: do current strategies need revision? Star 1993;52:1-3), and call for simplified approaches. Indeed, the evaluation team recommended that the approaches be simplified prior to the development of the national program in China and that aspects such as the follow up of patients each month for acute neuritis be focused on those patients at greatest risk. Simplification of disability recording is important, and recording should be directly related to action. The integration of the program is also important, as is a patient-based approach. This was a special study and is likely to be subject to a Hawthorne effect (the effect, usually positive, of being under study upon the person being studied) so that expanded implemention of this disability prevention program may not be quite as successful as these pilot projects have been. There are also particular aspects of the leprosy program in China, such as its vertical structure and level of manpower, which may make it difficult to replicate in other countries. Nonetheless, this study has shown that disability prevention programs can result in prevention of impairment and very substantial reductions in cracks and wounds in both the hands and feet.
(Note: The questionnaires and assessment forms used in this project are available upon request from Dr. Smith.)
Acknowledgment. We would like to thank the very large numbers of patients and staff in each of the eight project areas who worked very hard to make this program successful. We also thank The Leprosy Mission International and the Ministry of Public Health for their support and for providing the resources for this work. We would like to mention the inspiration of the late Mr. Bill Edgar (The Leprosy Mission International) and of Professor Dai Zhicheng (Ministry of Public Health, Beijing) in setting up this project.
REFERENCES
1. BECX-BLEUMINK, M. and BERHE, D. Occurrence of reactions, their diagnosis and management in leprosy patients treated with multidrug therapy. Int. J. Lepr. 60(1992)173-184.
2. ILEP. Prevention of disability: guidelines for leprosy control programmes. London: Calvert Press, 1993.
3. NAAFS, B., PEARSON, J. M. H. andWHEATE, H. W. Reversal reaction: the prevention of permanent nerve damage. Comparison of short and long term steroid treatment. Int. J. Lepr. 47(1979)7-12.
4. PALANDE, D. D. Nerve involvement in leprosy. Prevention and management of deformities: need for a paradigm-shift. Lepr. Rev. 65(1994)161-164.
5. PEARSON, J. M. H. and Ross, W. F. Nerve involvement in leprosy-pathology, differential diagnosis and principles of management. Lepr. Rev. 46(1975)199-212.
6. SMITH W. C. S. and JESUDASAN K. The elimination of leprosy and prospects for rehabilitation. Lancet 341(1993)89-90.
7. SMITH W. C. S., PARKHE S. M. Disability assessment as a measure of progress in leprosy control. Lepr. Rev. 57(1986)251-259.
8. SOMMERFELD, P. Voluntary donor agencies in antileprosy work: present contribution and probable future. Lepr. Rev. 64(1994)1-8.
9. SRINIVASAN, H. Prevention of disabilities in patients with leprosy. Geneva: World Health Organization, 1993.
10. WATSON, J. M. Disability control in a leprosy control programme. Lepr. Rev. 60(1989)169-177.
11. WORLD HEALTH ORGANIZATION. Progress towards eliminating leprosy as a public health problem. Wkly. Epidemiol. Rcc. 20(1994)145-151.
12. WORLD HEALTH ORGANIZATION. Progress towards eliminating leprosy as a public health problem. Wkly. Epidemiol. Rec. 21(1994)153-157.
13. ZHANG, G. C, LI, W. H., YAN, L. B., YANG, Z. M., CHEN, X. S., ZHENG T. S. and YE G. Y. Anepidemiological survey of deformities and disabilities among 14, 257 cases of leprosy in 11 counties. Lepr. Rev. 64(1993)143-149.
1. M.D., Department of Public Health, University of Aberdeen, Aberdeen AB9 2ZD, Scotland, U.K.
2. M.D., China Academy of Medical Science, Nanjing, People's Republic of China.
3. M.D., China Academy of Medical Science, Nanjing, People's Republic of China.
4. F.C.S.P., The Leprosy Mission International, London, U.K.
5. M.P.H., American Leprosy Missions, Belo Horizonte, Brazil.
6. M. D., Royal Tropical Institute, Amsterdam, The Netherlands.
Reprint requests to Dr. Smith at address above or Tel. 44-1224-681818, FAX: 44-1224-662994, Email: w.c.s.smith@abdn.ac.uk
Received for publication on 2 June 1995; accepted for publication in revised form on 5 September 1995.
APPENDIX: DESCRIPTION OF THE INTERVENTION PROGRAMME, THE OBJECTIVES AND EVALUATION CRITERIA
1. Detection and treatment of neuritis-groups of patients in all project areas were monitored for neuritis by monthly assessments of motor and sensory function over a period of 2 years. Patients who had any motor change, or sensory change of at least 2 points were to be promptly treated with a standard course of steroids tailing off over a period of 6 months.
Objective: to detect and treat neuritis promptly and adequately.
Measures: neuritis rates, delay between detection and treatment, steroid treatment compliance.
2. Self care of eyes, hands, and feet-patients in all project areas who had nerve function loss were to be trained to develop a regular pattern of self care of eyes, hands and feet over a period of 2 years.
Objective: to develop the habit of self care in a fixed number of patients.
Measure: count number enrolled in project, staffassessed regularity of self care, change in conjunctivitis, and changes in cracks, wounds and bone loss in hands and feet.
3. Footwear programme-in all areas footwear was to be provided to patients with insensitive feet which was locally acceptable and had a 1 cm thick insole of 15 shore cushioning. Specialised shoes such as shoes with moulded insoles and shoe rockers were to be provided to those with deformed feet.
Objective: to provide footwear to patients with insensitive feet.
Measure: number of patients provided with footwear and distribution of footwear over the study period, acceptability and durability of footwear, and changes in cracks, wounds and bone loss.
4. ILEP sole wound study-this 3 year multicentre study had 2 centres in China which were included in this programme, one at Taixing and the other in Hubei. In this part a cohort of 100 patients with sole sensory loss, half of whom had sole wounds, were managed by self care training and surgical treatment where necessary and were followed up over 3 years for change in sole wounds and cracks.
Objective: reduce cracks and wounds and to provide a learning experience for management.
Measure: change in cracks, wounds and bone loss.
5. Management of complicated plantar ulcers-this was to be undertaken in 6 areas where patients with complicated sole wounds defined as lesions affecting structures deep to the skin. The management was to include patient education, social change, surgery, dressings and the use of moulded footwear.
Objective: to treat a fixed number of patients with complicated sole wounds.
Measure: change in wound count and bone loss.
6. Reconstructive surgery-a target of 1170 procedures was set to be carried out in 6 areas which had surgical facilities.
Objective: to conduct a fixed number of surgical procedures.
Measure: count number of procedures, measure lid gap and vision after lagophthalmos correction, functional changes and joint angles after tendon transfer surgery in the hands and feet.
7. Amputations-a survey prior to the programme estimated that 1500 patients required lower limb amputation because of grossly deformed feet, these were to be carried out in 5 different areas.
Objective: to perform amputations when indicated for severe foot deformity, squamous carcinoma, and at the request of the patients.
Measure: count the number of amputations performed.
8. Prosthesis-the provision of effective prostheses was guaranteed prior to amputation.
Objective: to provide artificial limbs to all patients after amputation.
Measure: count number of prostheses, stump wound counts, and assess use of prostheses.
9. Staffand patient training-based on action learning both on the job as well as in the classroom would be provided for all staff in each of the pilot project areas and patients would be trained in self care.
Objective: to train a fixed number of staff and patients.
Measure: count number of staffand patients trained, conduct practical and theoretic tests on the trained staff and patients.
10. Patient education-would be provided in all areas supported by locally produced booklets and posters to reinforce one to one teaching.
Objective: write, print and distribute teaching and training material for staffand patients.
Measure: identify these publications and assess their use.