- Volume 63 , Number 2
- Page: 195–201
Relapse after long-term follow up of multibacillary patients treated by WHO multidrug regimen
ABSTRACT
Thirty-five multibacillary (MB) leprosy patients were treated with 2 years of multidrug therapy (MDT) and followed up regularly for relapse. Relapse was defined as: a) an increase of the bacterial index (BI) by 2+ over the previous value from any single site of old lesions and b) the occurrence of definite new skin lesion(s) which demonstrated a higher BI than any pre-existing lesion. After a mean duration of 72.7 ±17.3 months of follow up per patient, seven relapses were diagnosed; the mean incubation period of relapse was 62.7 ± 18.7 months. The overall relapse rate was 20.0% (or 3.3 per 100 patient-years), very significantly higher than the figures obtained from the same group of patients analyzed 2½ years earlier, indicating that relapses occurred late (at least 5 ± 2 years) after stopping MDT. Further analysis indicated that the relapse rate was closely correlated with the bacterial load of the patient, occurring far more frequently among patients with a BI of >4.0 before MDT or with a BI of >3.0 at the end of MDT. To avoid the alarmingly high relapse rate, it is proposed that the duration of MDT be doubled to 4 years in patients with an average BI of >4.0 before MDT.RÉSUMÉ
Trente-cinq atteints de lèpre multibacillaire ont été traités pendant deux ans par polychimiothérapie (PCT) et suivis régulièrement pour la détection de rechute. Une rechute était défine comme: a) une augmentation de l'indice bactérien (IB) de 2+ par rapport à la valeur précédente à n'importe quel site d'une ancienne lésion et b) l'apparition de nouvelle(s) lésion(s) cutanée(s) bien définies montrant un IB plus élevé que n'importe quelle lésion pré-existante. Après une durée moyenne de 72.7 ± 1 7.3 mois de suivi par patient, sept rechutes ont été diagnostiquées; la période d'incubation moyenne de la rechute était de 62.7 ± 18.7 mois. Le taux global de rechute était de 20.0% (3.3 pour 100 personnes-années), significativement beaucoup plus élevé que les résultats obtenus à partir du même groupe de patients et analysés 2Vl ans auparavant, ce qui indique que les rechutes sont survenues tardivement (au moins 5 ± 2 ans) après l'arrêt de la PCT. Une analyse ultérieure a montré que le taux de rechute était étroitement correlé avec la charge bactérienne du patient, survenant nettement plus souvent chez les patients avec un IB >4.0 avant la PCT ou > 3.0 à la fin de la PCT. Afin d'éviter ce taux de rechute extrêmement élevé, il est proposé que la durée de la PCT soit doublée jusqu'à 4 ans pour les patients qui ont un IB > 4.0 avant la PCT.RESUMEN
Treinta y cinco pacientes con lepra multibacilar se trataron con poliquimioterapia durante 2 años y luego se mantuvieron bajo observación para establecer la frecuencia de recaídas. Una recaída se definió como: (a) un aumento en el índice bacteriano (131) por arriba de 2+ sobre los valores previos, y (b) la ocurrencia de nuevas lesiones dérmicas con 131 mayores que los de cualquier lesión preexistente. En un promedio de 72.7 ± 17.3 meses de seguimiento se diagnosticaron 7 recaídas; el periodo de incubación promedio de las recaídas fue de 62.7 ± 18.7 meses. La frecuencia global de recaída fue del 20% (3.3 por 100 pacientes-años), cifra significativamente más elevada que la reportada 2.5 años antes en el mismo grupo de pacientes. Esto fue indicativo de que las recaídas ocurrieron tardíamente, cuando menos 5 + 2 años después de suspender la PQT. El análisis ulterior indicó que la frecuencia de recaída correlacionó con la carga bacteriana del paciente, ocurriendo más frecuentemente entre los pacientes con un BI de >4.0 antes de la PQT, o en aquellos con un BI >3.0 al final de la PQT. Se propone que la duración de la PQT se extienda a cuatro años en los pacientes con un BI promedio de >4.0, con el fin de abatir la alarmantemente elevada frecuencia de recaídas.Introduction and implementation of multidrug therapy (MDT), which was recommended by a World Health Organization (WHO) Study Group (10) in 1982, are the most important developments in the history of leprosy control activities. Based on the size of bacterial populations, leprosy patients are classified into paucibacillary (PB) and multibacillary (MB); PB patients are treated with two drugs, rifampin (RMP) and dapsone (DDS), and MB patients with three drugs, RMP, DDS and clofazimine (CLO)(10). Although the duration of MDT for MB leprosy was recommended originally as a minimum of 2 years, or to be continued until skin-smcar negativity (10), the great majority of national leprosy control programs discontinue the treatment of MB cases after 2 years of MDT with highly effective results (1). Therefore, 2 years has been adopted recently as the routine duration of MDT for MB leprosy by the second WHO Study Group Meeting (9).
Up to 1993, more than 4 million leprosy patients in the world completed their treatment with MDT (11). Data from routine leprosy control programs indicated that, after completion of MDT, the relapse rates were well below 1% (1). In a questionnaire survey organized by WHO, 467 relapses were diagnosed among 92, 194 MB cases, with an overall relapse rate of 0.51%, or 0.23 per 100 patient-years (8). In another questionnaire survey, 67 relapses were diagnosed among 20, 141 MB cases observed during the period 1984-1992 (with a mean duration of follow up about 4 years per patient), the cumulative risk of relapse was 0.77% at the end of 9 years after stopping MDT, and the annual rate of relapse ranged from 0.01% to 0.14% (8). However, the low relapse rate must be interpreted with great caution because the durations of follow up in the majority of the patients were relatively short; whereas the relapses after treatment with any RMP-containing regimens occurred late, at least 5 ± 2 years after stopping treatment (4). Further accumulation of relapse data is necessary for the assessment of the longterm therapeutic effect of MDT.
In our previous report, we have reported that in a group of MB patients treated with 2 years of MDT the overall relapse rate was 2.9%, or 0.8 per 100 patient-years (4). Because the results were obtained only after 41.9 ± 12.1 months of follow up, we emphasized the need to continue following up these patients (4). After an additional 2Vi years of follow up, the overall relapse rate of the group has increased tremendously, to 20.0% or 3.3 per 100 patient-years. To cope with such an alarmingly high relapse rate, we believe that action in preventing relapse should be and could be taken, because we have observed a clear correlation between relapse and the size of the bacterial population in patients before and at the end of MDT.
PATIENTS AND METHODS
Patients. Between 1984 and 1986, 75 MB patients were admitted to the Institut Marchoux and were treated for 2 years with the WHO/MDT regimen (4). Patients were hospitalized until completion of therapy. All drugs, including daily DDS and CLO, were administered under supervision by medical personnel. Of the 75 cases, only 44 completed the scheduled treatment. Among those 44, 9 were not suitable for analysis of relapse: 6 had never returned for follow-up examination by the end of March 1994 and 3 had been seen only during the first 12 months after completing MDT. Thus, only 35 cases have been seen at least once later than 12 months after completing treatment, and are eligible for analyzing the relapse rate (4).
Before starting MDT, 14 of the 35 cases had never received antileprosy treatment, 15 had been treated for various durations with DDS monotherapy, 5 with DDS monotherapy followed by various durations of DDS plus RMP, and 1 with 6 months of treatment with a combination of RMP, DDS and CLO. All 35 cases had multiple, active, MB leprosy skin lesions (such as diffuse infiltration, erythema, macule, plaque, nodule or leproma) and their Mitsuda reactions to the lepromin test were all negative, i.e., <3 mm in diameter. Based on histopathological examination of skin biopsies, 6 cases were diagnosed as polar lepromatous (LL) and 29 as borderline lepromatous (BL) leprosy by the Ridley-Jopling classification (6). On Ridley's scale (5), the average bacterial index (BI) calculated from all (normally six) sites of skin smears ranged from 1.0 to 5.2, and 18 cases had an average BI of > 4.0. All 35 cases had a maximum BI, i.e., the highest BI among the smear sites of >2 + , and 28 had a maximum BI of >5 + . The morphological index (MI) of the bacilli was >1 % in 27 cases. After 2 years of MDT, active skin lesions disappeared from all cases. However, skin smears were still positive, except in cases 177, 197, 213 and 240, but their Mis became zero.
Follow up. After completion of MDT, whenever patients came to the clinic a thorough physical examination was carried out, with special emphasis on the evolution of pre-existing leprosy lesions and detection of suspected new lesions. A urine specimen was collected for DDS analysis, and skin smears were taken from the same sites originally examined, if no such examination had been performed within the last 12 months, and from any suspected new lesion(s).
Relapse was suspected if the BI at any site was found to have increased by at least 2 + over the previous value, and/or occurrence of any active skin lesion with a BI greater than that in any pre-existing lesion. Further examinations included repeating the physical examination, retesting the skin smears, and taking a biopsy from the suspected lesion for histopathological examination, and for testing the viability and drug (RMP, DDS and CLO) susceptibility of the organisms by mouse foot pad inoculation (4). Relapse was diagnosed if two of the following three criteria were met: a) a significant increase of the BI, i.e., by at least 2+ over the previous value, at any site was confirmed; b) the occurrence of a definite new skin lesion; and c) demonstration of viable organisms by mouse foot pad inoculation (2,4).
Statistical analysis. In calculating the overall relapse rate and relapse rate per 100 patient-years, the number of relapsed cases after stopping MDT was used as the numerator, the number of patients eligible for analysis of relapse and their total duration of follow up, in terms of patient-years, were used respectively as denominators. The incubation period of relapse after completion of MDT was calculated as the number of months between stopping treatment and the appearance of relapse, and date of relapse was defined as the midpoint between the dates of the last examination without relapse and the first examination revealing evidence of relapse (4). Results were analyzed by Fisher's exact probability calculation and the Student's / test. Differences were considered significant at the 95% level of confidence.
RESULTS
Of the 35 cases eligible for analysis of relapse, 29 (82.9%) had been followed up at least 5 years, and 17 (48.6%) for more than 7 years. By the end of March 1994, the total duration of follow up was 212 patient-years, or the mean duration of follow up was 72.7 ± 17.3 months per patient. During followup examinations, a urine analysis for DDS was virtually negative in all cases, indicating that this group of patients had, indeed, stopped chemotherapy since completion of MDT.
The mean value of the average Bis of these patients was 3.80 ± 1.09 before starting MDT, and significantly declined to 2.16 ± 1.57 by the time of completion of MDT (p <0.05). The BI continued to decline in almost all cases despite stopping chemotherapy, and had reached negativity at least once during the course of follow up in 27 (77.1%) cases. However, the Bis rebounded or became positive again, accompanied by new skin lesion(s) in seven cases (The Table).
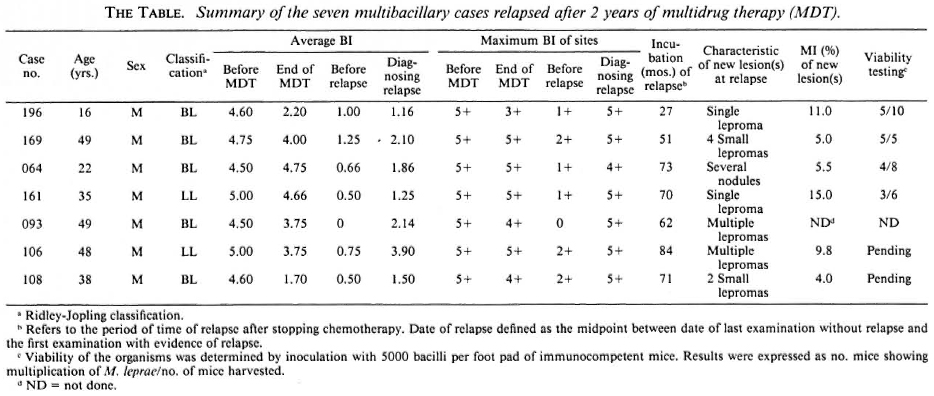
The overall relapse rate was 20.0% (3.3 per 100 patient-years), very significantly greater than the figures obtained 2 ½ years earlier from the same group, 2.9% and 0.8 per 100 patient-years, respectively (4). As shown in The Table, the incubation period of relapse varied among the seven relapses: 1 relapsed in the third year after stopping MDT, 1 in the fifth year, 4 in the sixth or seventh year, and 1 at the beginning of the eighth year, which is the maximal possible duration of follow up in the group. The mean incubation period of relapse was 62.7 ± 18.7 months after completion of MDT, a figure very similar to that of relapses after stopping treatment with other RMP-containing combined regimens (4).
The pre-MDT characteristics of the relapsed cases, including age, male/female ratio, classification of leprosy, and history of previous treatment, did not differ significantly from those of nonrelapsed cases. The major difference between the two subgroups is that the relapsed cases had significantly greater bacterial loads, in terms of average BI in skin smears, before and also at the end of MDT. The mean value of the average Bis before and at the end of MDT was, respectively, 4.71 ± 0.22 and 3.57 ± 1.17 in the seven relapsed cases, significantly greater than the corresponding figures in the 28 nonrelapsed cases, 3.58 ± 1.10 and 1.80 ± 1.46 (p <0.05, p <0.01), respectively. In addition, the average BI before MDT was > 4.0 in 18 cases and <4.0 in 17 cases; 7 (38.9%) of the former but 0 of the latter group relapsed (p <0.01); the average BI at the end of MDT was >3.0 in 12 cases and <3.0 in 23 cases, 5 (41.7%) of the former and 2 (8.7%) of the latter group relapsed (p <0.05). These results suggested that the relapse rate was closely correlated with the bacterial load, and relapse was significantly more frequent among patients with a BI of >4.0 before MDT or a BI of >3.0 at the end of MDT.
Among the seven relapsed cases, the average Bis continued to decline after stopping MDT, as in the nonrelapsed cases, and had become negative at least once in two cases (nos. 093 and 108). The mean value of the seven cases had reached 0.67 ± 0.40 at the last examination without evidence of relapse. By the time relapse was diagnosed, the mean value of the average Bis rebounded to 1.99 ± 0.93; the maximum Bis among the smear sites of each patient were mostly 5 + , an increase more obvious than the increase in the average BI.
When relapse was diagnosed, 5 of the 7 cases only had a single or a few small nodules or lepromas. Although the number of new lesion(s) was small, they always had a high BI, mostly 5 + , and a high MI, 8.4% ± 4.3% (The Table). The small number of new lesion(s) suggested that the diagnosis of relapse was relatively early and, therefore, the estimation of the incubation period of relapse may be quite close to the actual one. The small number of new lesions also explains the reason why the increase in the average BI was less obvious than the increase in the maximum BI of the skin smears.
Skin biopsies were taken from six of the relapsed cases; biopsy was refused by case 093. The bacilli recovered from the biopsies were inoculated into foot pads of mice for testing the viability and drug (RMP, DDS and CLO) susceptibility of the organisms. To date, the results of organisms recovered from four patients are available, and all demonstrate the presence of viable organisms in the inoculum, i.e., 5000 bacilli per mouse foot pad. Three isolates were resistant to DDS (cases 169, 064 and 161) but none of the four isolates were resistant to RMP or CLO, suggesting that the DDS-resistance emerged before the administration of MDT.
DISCUSSION
Because leprosy is such a chronic disease and relapse occurred late after treatment with any RMP-containing regimens (4), it is understandable that to date (10 years after the introduction of MDT) data about the relapse rate of MDT are still very limited. However, as in the case of other infectious diseases, after cessation of specific antimicrobial treatment, the relapse rate among MB leprosy is a crucial parameter in assessing the long-term efficacy of chemotherapy in leprosy.
After 2 years of MDT, skin smears are still positive in a significant proportion of MB patients when the treatment is stopped. As a result, the demonstration of acid-fast bacilli in skin smears alone is no longer sufficient for the diagnosis of relapse as it was during the era of DDS monotherapy. Therefore, relapse may now be diagnosed only according to more stringent criteria: a) an increase in the BI of > 2 + over the previous value from any single site of old lesions; b) the occurrence of definite new skin lesion(s) which demonstrate a higher BI than any pre-existing lesion; and c) the demonstration of viable organisms by mouse inoculation, an indicator of bacterial remultiplication (4). However, because the facilities for mouse inoculation are not accessible by most leprosy control programs, and because viable organisms were demonstrated in nearly 90% of the clinically relapsed cases in the previous study (4), we believe that the first two criteria are sufficient for the diagnosis of relapse under field conditions. In theory, relapse may occur in the absence of obvious new lesion(s) during its early stage but, in our experience, new lesion(s) must occur sooner or later in real relapse. Because the quality of skin smears is far below that which is desirable in many leprosy control programs, if the increase in the BI is not accompanied by new lesion(s), we propose that the patient be kept under close surveillance and be examined repeatedly every 3 to 6 months. After all, in most cases, relapse is not a clinical emergency, and there is no need to make a quick decision.
Based on the above-mentioned criteria, seven relapses were diagnosed in the current study. Because the mean incubation period of the observed relapses of 62.7 ± 18.7 months was close to the mean duration of follow up in the group, 72.7 ±17.3 months, it leads to the suspicion that more relapses will occur as the follow up is prolonged. It is, therefore, reasonable to believe that in this group a 20.0% overall relapse rate or 3.3 per 100 patient-years are the minimal figures of eventual relapse after 2 years of MDT, very significantly greater than those obtained from the questionnaire surveys (8). Because the relapse rate increased tremendously when the duration of follow up was extended from 41.9 ± 12.1 months to 72.7 ± 17.3 months, and also because the mean incubation period of the observed relapses was 62.7 ± 18.7 months, we believe that relapse occurred late, at least 5 ± 2 years after stopping MDT, as in the case treated with other RMP-containing combined regimens.
After further analysis, it is clear that the relapse rate was closely correlated with the bacterial load of the patient before or at the end of MDT: 38.9% and 41.7% relapsed, respectively, among patients who had an average BI of >4.0 before MDT or >3.0 at the end of MDT; whereas the relapse rate was, respectively, 0% and 8.7% among patients who had an average BI of < 4.0 before MDT or <3.0 at the end of MDT. MB cases with an average BI of >4.0 before MDT are relatively few in the field where MDT is implemen-ted. This could be the explanation for the overall relapse rate being low in the field even after a longer duration of follow up than the present (8). Nevertheless, in reference centers, e.g., Institut Marchoux where the current study was carried out, patients with a high bacterial load are still encountered regularly, which explains why the relapse rate in reference centers may be significantly higher than that in the field.
The fact that no RMP resistance has been demonstrated among 50 strains isolated from relapsed cases in the previous (4) and current study, and relapse was closely correlated with the bacterial load of the patient, suggests that relapses in these patients were not caused by the emergence of drug resistance but probably by Mycobacterium leprae persisters (7). The results of the earlier study suggested that the number of persisters may be higher in patients with a higher bacterial load (7), and the results of the current study suggest that higher number of persisters may lead to greater risk of relapse.
To avoid the high relapse rate after stopping MDT treatment, as observed in the current study, it is suggested that the duration of MDT be prolonged in patients with an average BI of > 4.0 before MDT or >3.0 at the end of MDT. Taking into account the difficul-ties in organizing skin-smear service with desirable quality under field conditions, it is not feasible to repeat skin smears on a regular basis and, therefore, it might not be feasible to use the average BI at the end of 2 years of MDT as an indicator for the duration of treatment. On the other hand, the average BI of >4.0 before MDT may be more practical as an indicator because skin smears are routinely taken from every case before MDT is given, and this indicator does not require that skin smears be repeated regularly. Because the rate of decrease of an average BI is about 0,6 units per year in high BI cases, in order to reduce the average BI to a level well below 3.0 by the end of MDT, the duration of MDT may need to be doubled to 4 years in patients with an average BI of >4.0 before MDT.
Another point of view would be that, taking into account that MB patients with an initial average BI of >4.0 are relatively few in the field, the total number of relapses in a control program should be small. Since the great majority of relapsed cases would be expected to remain susceptible to RMP and CLO and it would require tremendous efforts to upgrade the quality of skin-smear service which is crucial for detecting patients with a BI of >4.0, it could be suggested, from an operational point of view, that any control program should accept that relapse may eventually occur from a certain proportion of patients with an initially high BI and, consequently, it is not necessary to introduce a lengthy duration of MDT for a small number of these particular cases.
REFERENCES
1. ALM CONSENSUS DEVELOPMENT CONFERENCE ON THE CHEMOTHERAPY OF LEPROSY. Consensus development statement on the chemotherapy of leprosy. Int. J. Lepr. 60(1992)644-652.
2. JAMET, P., BLANC, L., FAYE, O. C, TRAORE, I. and BOBIN, P. Relapses after a single dose of rifampin in skin-smear negative multibacillary patients after dapsonc monotherapy. Int. J. Lepr. 62(1994)209-214.
3. Ji, B. and GROSSET, J. Recent advances in the chemotherapy of leprosy. (Editorial) Lepr. Rev. 61(1990)313-329.
4. MARCHOUX CHEMOTHERAPY STUDY GROUP. Relapses in multibacillary leprosy patients after stopping treatment with rifampin-containing combined regimens. Int. J. Lepr. 60(1992)525-535.
5. RIDLEY, D. S. and HILSON, G. R. F. A logarithmic index of bacilli in biopsies. Int. J. Lepr. 35(1967)184-193.
6. RIDLEY, D. S. and JOPLING, W. H. Classification of leprosy according to immunity; a five-group system. Int. J. Lepr. 34(1966)255-273.
7. SUBCOMMITTEE ON CLINICAL TRIALS OF THE CHEMOTHERAPY OF LEPROSY (THELEP) SCIENTIFIC WORKING GROUPOFTHE UNDP/WORLD BANK/ WHO SPECIAL PROGRAMME FOR RESEARCH AND TRAINING IN TROPICAL DISEASES. Persisting Mycobacterium leprae among THELEP trial patients in Bamako and Chingleput. Lepr. Rev. 58(1987)325-337.
8. WHO LEPROSY UNIT. Risk of relapse in leprosy. WHO Document. WHO/CTD/LEP/94.1.
9. WHO STUDY GROUP. Chemotherapy of leprosy. Geneva: World Health Organization, 1994. Tech. Rep. Ser. 847.
10. WHO STUDY GROUP. Chemotherapy of leprosy for control programs. Geneva: World Health Organization, 1982. Tech. Rep. Ser. 675.
11. WORLD HEALTH ORGANIZATION. Progress towards the elimination of leprosy as a public health problem. Wkly. Epidemiol. Ree. 68(1993)181-188.
Reprint request to Dr. Jacques Grosset, Bactériologie et Virologie, Faculté de Médecine Pitie-Salpctriere, 91 Blvd. de l'Hôpital, 75634 Paris 13, France.
Received for publication on 13 December 1994.
Accepted for publication on 23 February 1995.
Members of the Marchoux Chemotherapy Study Group are: Leopold Blanc, Pierre Bobin, Denis Daumerie, Guy Discamps, Ousmane Cheik Faye, Jacques Grosset, Gerard Grossetete, Jean Alain Husser, Pierre Jamet, Baohong Ji, Antoine Mahe, Max Nebout, Stefaan Pattyn, Samba Sow, and Issa Traore.