- Volume 63 , Number 2
- Page: 291–3
Mast cells in lepromatous leprosy
To the Editor:
Leprosy is a chronic disease, caused by Mycobacterium leprae, which is characterized histologically by granuloma formation. The type of granuloma depends upon the cellular-immune response of the host to the organism (8). Apart from the usual cells which participate in the granuloma, such as epithelioid cells, macrophages and lymphocytes, mast cells also have been observed in the lesion. It has been noted that the numbers of mast cells in lesions of lepromatous leprosy are more compared to those of tuberculoid leprosy (1). The purpose of this study is to study the role of mast cells in treated and untreated cases of lepromatous leprosy.
Skin biopsies from 21 patients with lepromatous leprosy were reviewed. Classification of leprosy was according to the criteria of ridley and jopling (9). Sections cut from paraffin-embedded material were stained with hematoxylin and cosin (H&E) and Fite's stain for acid-fast bacilli (AFB). Two additional serial sections from each case were stained with the chloracetate esterase (Pararosanilin) method to detect mast cells (2). Granules of mast cells were stained pinkish red. The number of mast cells in the entire biopsy tissue was counted using a light microscope (Olympus) under a x 100 objective (oil immersion). The final mast cell count was obtained by averaging the numbers of mast cells in the two serial sections of the biopsy. The density of the mast cells was expressed as the number of cells/ mm2. The Mann-Whitney U test was used to compare the mast cell numbers in two groups of lepromatous leprosy cases (untreated and treated).
The clinical data of the patients and the density of mast cells in the skin lesions are given in Tables 1 and 2. H&E sections of lesions of untreated leprosy cases revealed macrophage granulomas containing numerous solid AFB. Biopsies of treated cases showed vacuoles in the macrophages. AFB staining exhibited mainly fragmented bacilli.]
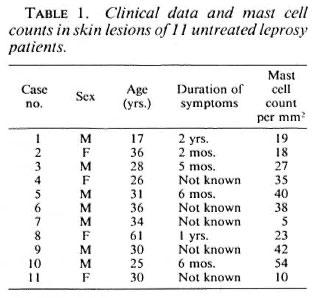
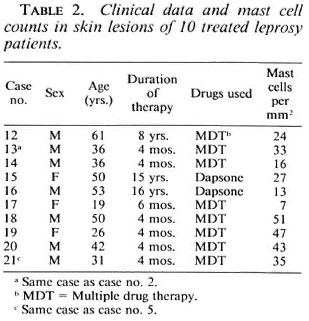
There were no statistically significant differences between the mast cell counts in treated and untreated lepromatous groups (p = 0.83).
Mast cells play an important role not only in immediate hypersensitivity reactions but also in delayed hypersensitivity reactions (5). Mast cells are activated by cytokines such as interleukin-3 (IL-3) and IL-4 produced by the activated T cells (3). The T-cell-mediated immune response plays a major part in leprosy. A study of cytokine patterns and T-cell subsets in leprosy has been done, showing that in lepromatous lesions, typical Th-2 cytokines are high, one of which is IL-4 (11). On the other hand, reactive T cells from tuberculoid patients were of the Th-1 phenotype, and these cells produce undetectable levels of IL-4 (6). Several researchers (1, 7, 10) have observed the predominance of mast cells in lepromatous leprosy lesions as compared to those oftuberculoid leprosy. One would speculate that with chemotherapy the density of mast cells in lepromatous lesions would reduce. However, in the present study no significant difference in mast cell density was noted between treated and untreated lepromatous lesions. This is probably due to two reasons. Firstly, the life span of mast cells is long, ranging from weeks to months (7). In our study, skin biopsy in 7 of the 10 patients in the treated group was done within 6 months of chemotherapy. Perhaps 6 months is too short a period to expect reduction in the the mast-cell density in the lesions. Secondly, it is possible that reduction of mast cell density occurs only when the lesions upgrade to become more of the tuberculoid type, with changes in the cytokine pattern. We did not note any upgrading of the lesions in the treated group. The histology of the lesions in the treated group showed vacuolated macrophages containing fragmented bacilli, indicating only a response to chemotherapy.
- Pailoor Jayalakshmi, M.Path.,
M.R.C. Path.
Associate Professor
- Tan Kim Lian
Medical Technologist
Department of Pathology
Faculty of Medicine
University of Malaya
59100 Kuala Lumpur, Malaysia
REFERENCES
1. ARONI, K., KONTOCHRISTOPOULOS, G., LIOSSI, M. and PANTELEOS, D. An investigation of mast cells in two basic leprosy groups. Int. J. Lepr. 61(1993)634-635.
2. BANCROFT. J. D. Enzyme histochemistry. In: Theory and Practice of Histological Techniques. 3rd edn. Bancroft, J. D. and Stevens, A., eds. Edinburgh: Churchill Livingstone, 1990, pp. 406-407.
3. COTRAN, R. S., KUMAR, V. and ROBBINS. S. L. Diseases of immunity. In: Robbins Pathologic Basis of Disease. 4th edn. Philadelphia: W. B. Saunders Company, 1989, pp. 163-237.
4. GALLI, S. J. New concepts about mast cells. N. Engl. J. Med. 328(1993)257-265.
5. GALLI, S. J. and DVORAK, A. M. What do mast cells have to do with delayed hypersensitivity? Lab. Invest. 50(1984)365-368.
6. HAANEN, J. B. A., DE WAAL-MALEFUT, R., RES, P. C. M., KRAAKMAN, E. M., OTTENHOFF, T. H. M., DE VRIES, R. R. P. and SPITS, H. Selection of a human T helper type 1 -like T cell subset by mycobacteria. J. Exp. Med. 174(1991)583-592.
7. RAV, S. D., PRATAP, V. K., SHARMA, N. K. and DAYAL, S. S. Mast cells in leprosy. Indian J. Lepr. 62(1990)467-472.
8. RIDLEY, D. S. Histological classification and the immunological spectrum of leprosy. Bull. WHO 51(1974)451-465.
9. RIDLEY, D. S. and JOPLING, W. H. Classification of leprosy according to immunity; a five-group system. Int. J. Lepr. 34(1966)255-273.
10. VAN HALE, H. M., TURKEL, S. B. and REA, T. H. Dermal ultrastructure in leprosy. Arch. Pathol. Lab. Med. 108(1984)383-386.
11. YAMAMURA, M., UYEMURA, K., DEANS, R. J., WEINBERG, K., REA, T. H., BLOOM, B. R. and MODLIN, R. L. Defining protective responses to pathogens; cytokine profiles in leprosy lesions. Science 254(1991)277-279.