- Volume 63 , Number 1
- Page: 23–7
Doppler sonography of vertebral arteries and audiovestibular system investigation in leprosy
ABSTRACT
Thirty-six patients with leprosy and 12 sex- and age-matched controls were investigated for disorders of the audiovestibular system, and vertebral artery measurements were calculated using a color Doppler ultrasound technique. Sensorineural hearing loss found to be of cochlear origin was detected in 8 of the leprosy patients. Maximal flow velocity and mean flow velocity were measured, and the total vertebral artery flow was calculated by adding flows F rom the right and left sides. There was a significant reduction in the total maximal peak flow velocity of the vertebral artery of the lepromatous patients compared to the controls. Dopplcr sonography of the vertebral artery gave useful information about some pathology seen in lepromatous patients.RÉSUMÉ
Trente-six patients lépreux et 12 témoins appariés pour le sexe et l'âge ont été examinés pour la recherche de désordres du système audio-vestibulaire, et les mesures de l'artère vertébrale ont été calculées par une technique à ultra-sons de Dopplcr. Une perte d'audition sensori-nerveuse d'origine cochléaire a été trouvée chez huit des malades de la lèpre. La vélocité maximale en flux et la vélocité moyenne ont été mesurées, et le flux total de l'artère vertébrale a été calculé en additionnant les flux des côtés gauche et droit, Il y avait une différence significative entre le pic maximum total de vélocité de l'artère vertébrale des patients lépromateux et des témoins. La sonographic Dopplcr de l'artère vertébrale a donné des informations utiles à propos de certaines pathologies observées chez des malades delà lèpre.RESUMEN
Treinta y seis pacientes con lepra y 12 controles de su misma edad y sexo se sometieron a estudios para buscar desórdenes del sistema audiovestibular. También se hicieron mediciones en la arteria vertebral usando la técnica de sonografia de Dopplcr. Se encontró una pérdida scnsoncural auditiva de origen coclear en 8 de los pacientes con lepra. Se midieron tanto la máxima velocidad de flujo como la velocidad media de flujo. El flujo total de la arteria vertebral se calculó adicionando los flujos de los lados derecho c izquierdo. Hubo una diferencia significativa en la velocidad del flujo máximo de la arteria vertebral entre los pacientes lepromatosos y los controles. La sonografia de Dopplcr de la arteria vertebral proporcionó información útil sobre la patología de los pacientes lepromatosos.Leprosy is a systemic infectious disease which has a predilection for the skin, peripheral nerves, and mucosa of the upper respiratory tract (3). In addition, the autonomic nervous system and arterial vasculature are affected in leprosy (7,12). To date, investigations of auditory function have shown that various elements of the auditory apparatus have been implicated in the mechanism of hearing loss in those with leprosy (l7). It has been reported that hearing loss was considered to be of cochlear origin but the cause of the cochlear pathology in leprosy is not clear (12).
Two vertebral arteries (VA), the basilar artery (I3A) and their branches supply blood to the brain stem, cerebellum and medulla containing the vestibular and cochlear nuclei and the labyrinth. If a dominant VA is occluded, then blood flow to these nuclei and the labyrinth may be diminished markedly and cochleo-vcstibular symptoms may occur (,6). Doppler ultrasonography of the cervical vessels and vertebral artery has made the detection of even a small vascular lesion possible. In 1965, Miyasaki and Kato l4) reported a Doppler ultrasound recording of the blood flow velocity in the external arteries supplying the brain and the labyrinth. This technique is a safe and noninvasive method, and gives information about the above-mentioned arteries.
The aim of this study is to investigate the flow of the vertebral arteries in lepromatous leprosy patients and to detect the possible cause of the cochleo-vestibular pathology which occurs in leprosy.
MATERIALS AND METHODS
The study was performed on 36 patients with leprosy aged 30 to 56 years (27 males and 9 females; average age, 42 years). Twelve age- and sex-matched normal individuals attending an car, nose and throat clinic were assessed as controls. Thirty-two patients had lepromatous leprosy; 4 patients, the tuberculoid form. The maximum duration of the disease was 43 years; minimum, 7 years; mean duration, 28 years.
Systemic, neurological and otorhinolaryngological examinations were made. Tuning fork tests, pure tone audiometry (interacoustics, AC 5 clinical computed audiometer), and tests of stance and gait were done with relevant techniques (9).
Color Doppler ultrasound flow imaging examinations were performed using ATL 5 MHz linear array transducers and both vertebral arteries were tested simultaneously. The subjects were placed in a supine position. The extracranial portion of the vertebral artery was explored behind the mastoid, and the probe was positioned in a vertical depression 1 cm underneath and posterior to the mastoid, behind the occipital head of the sternocleidomastoid muscle. A good-quality Doppler spectrum was obtained and the measured mean velocities were averaged. This measurement gave a time-average velocity of the flow through the vessel. The internal lumen diameter was determined. From this diameter, a crosssectional area was calculated that, when multiplied by the time-average velocity, gave a quantitative flow in milliliters per minute in the vessel. The peak velocity of the flow was measured. The vertebral artery flow was assessed in the right and left vertebral arteries in both leprosy patients and controls.
RESULTS
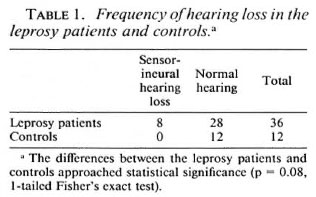
Thirty-six lepromatous patients were examined and 8 (22.2%) were found to have sensorineural hearing loss. Of these 8 patients, 4 had mild (27-40 dB hearing loss for both air and bone conduction), 3 had moderate (41-55), and 1 had severe (71-90 dB) sensorineural hearing loss. There was no hearing loss in the control group (p = 0.008; Table 1). In the hearing loss group, the speech detection threshold was lower than normal, the tone-decay test showed 0-25 dB, and the Met/, recruitment test was positive in 7 patients. These findings were normal in the controls.
Caloric test results in 36 patients showed 4 abnormal values; 2 patients were found to have canal paresis, the other 2 ears could not be stimulated by hot or cold air stimuli.
Spontaneous nystagmus was demonstrated in 4 patients, and abnormalities in postural tests were demonstrated in 2 patients; 1 was found to have a positive Romberg, the other had a positive Untcrbcrger's test. These test findings were normal in the control group.
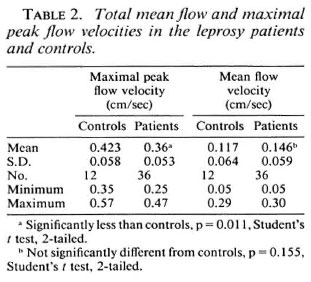
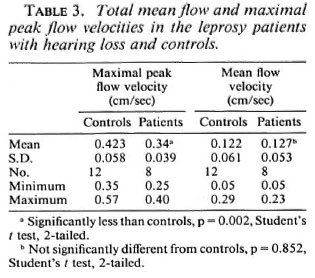
Vertebral artery hemodynamics, mean flow velocity and maximal peak velocity, were assessed first by individually measuring the flow in the right and left vertebral arteries and then adding these two values together to give a total or net vertebral artery flow. The results of the vertebral artery hemodynamics were compared with the right and left side and also with the controls (Table 2). There was a statistical significance when comparing the total maximal peak flow velocity of the vertebral artery of the lepromatous patients and the controls (p = 0.011). Although there were no statistically significant differences between the leprosy patients with and without hearing loss with respect to their results of total mean flow velocity and maximal peak flow velocity, there was a statistically significant difference between the total maximal peak flow velocity of the lepromatous patients with hearing loss and the controls (p = 0.002; Table 3). Six (75%) of the 8 patients with sensorineural hearing loss were found to have both abnormal hearing tests and abnormal vertebral flow velocities.
DISCUSSION
The possibility of a relationship between hearing loss and leprosy was proposed by Latif (13) and is reported to be a gradual and progressive hearing loss in 11% of a series of 101 leprosy patients, a few of whom also were found to have vestibular dysfunction (10). Audiograms on patients with Hansen's disease are interpreted as specific evidence of cochlear and acoustic nerve damage, and are reported to show decreases in the range of bone conduction in 52% of patients, vestibular involvement in 31 %, and nystagmus in a few patients (6,l8).
In our study, although the difference in the rates of hearing loss between the two groups is not statistically significant (which could be due to the small number of controls, N = 12), there was an increase (22%) in the rate of sensorineural hearing loss in the leprosy group. Tone decay and Mctz recruitment tests suggested that the hearing loss was of cochlear origin rather than a direct involvement of the acoustic nerve. No attempts have been made to demonstrate the presence of Hansen's bacillus in the inner car or in the acoustic nerve because our leprosy patients are still alive. Etiologic factors that could explain this hearing loss in leprosy have been investigated. The ages of the patients with hearing loss were younger (mean 43 years). Therefore, senility as the cause of the sensorineural hearing loss in the eight patients is not a factor. Another possible cause, streptomycin, was received by only two patients (7.2%) as part of their treatment. The administration of the drug was irregular and, also, no hearing loss was found in these two patients who had received streptomycin. The rest of the patients received dapsone preparations, which are not known to have any side effects on hearing or on the eighth nerve.
Caloric testing demonstrated vestibular abnormality in 11% of the leprosy group; 2 of these patients demonstrated unilateral weakness, in another 2 no stimulation of the canal was achieved. In addition, 5.6% of the leprosy patients had abnormalities on postural testing (positive Romberg and Unterberger tests).
Central nervous system involvement has been described, and the impairment of both parasympathetic and sympathetic functions has been demonstrated in lepromatous patients (11,12). The sympathetic damage was always associated with parasympathetic damage, and the severity of the autonomic neuropathy was found to be higher in those having leprosy for a longer duration. It has been reported that the incidence of autonomic neuropathy in a series was from 14.3% to 57% for various tests (15).
It has been thought that arterial involvement in leprosy was frequent and that the vessels in leprosy showed smooth tapering, absence of collaterals, and occlusion of vessels. Sixty arteriograms were done in 20 lepromatous leprosy cases and these lesions were seen in 25% of the cases (7). It has been reported that decreased blood flow through the arteries can lead to ischemia, and artériographie findings are directly proportional with the age of the patient and the duration of the plantar ulcer (18 ).
Doppler ultrasonography might be able to identify a group of patients who, with normal cerebral vasculature or only mild anatomic disease, have abnormal hemodynamic function that might contribute to their disease (4). Doppler ultrasonography also may provide a valuable diagnostic method of detecting abnormal hemodynamics to determine the potential for such ischemia. Strong vertebral artery flow often is associated with severe cerebrovascular disease in other vessels. In normal artery flows, the mean peak velocity will range from 20 to 40 cm per second; in cases of significantly diminished flow, this value will typically be less than 10 cm per second (5). Functionally, such measurements should provide additional insights into the performance of the vertebrobasilar system. These data suggest that these symptoms may relate to inadequate vertebral artery blood flow 5). There are many reports in the literature about the reliability of Doppler sonography in the diagnosis of stenotic lesions in the vertebral artery. Some of the questions of reliability may be related to recordings from the vertebral arteries being made with different techniques and at different anatomic levels.
In lepromatous patients, the velocity of blood flow in the cutaneous lesions was measured by laser Doppler velocimetry and was found to be slightly faster over the lesion than in adjacent uninvolvcd skin. There was relatively little difference between measurements at the edge and center of individual plaques or between the plaques in the same patient, but there were considerable differences between patients. Laser Dopplcr vclocimetry might be prove to be a useful, clinically acceptable, noninvasive technique for monitoring the severity of hyperemia (2).
In the present study, we examined the vertebral arteries simultaneously at the level of the submastoid region with a color Doppler ultrasound technique. Total maximal peak flow velocities in the vertebral arteries of the lepromatous patients were lower than in the controls. We also have found a significant difference between the total maximal peak flow velocities of the lepromatous patients with hearing loss and the controls. In contrast, we could not detect any difference between the total maximal flow velocities of the lepromatous patients, with and without hearing loss, with respect to their total mean flow velocities.
Diminished blood flow of the vertebral artery affects the nutrition of the structures containing the vestibular and cochlear nuclei, the labyrinth and brain stem, etc. Some symptoms related to this structure may occur as a result of this malnutrition of this structure, including hearing loss, tinnitus, and dizziness, resulting from diminished blood flow to the cochleovestibular nuclei, the labyrinth or brain stem.
The blood flow of the vertebral artery may be greatly affected by such factors as lesions of the vertebral artery itself or autonomic nervous system pathology occurring in leprosy. Sensorineural hearing loss might be attributed to the disease process of leprosy because of the diminished flow to the cochlea. Lepromatous patients should be studied in a vertebral artery angiographic investigation and autonomic nervous system examination in order to detect the probable cause of this diminished blood flow.
REFERENCES
1. AGRAWAL, B.R. and AGRAWAL, R.I. Arteriography in leprosy. Indian J. Lepr. 57(1985)138-145.
2. AGUSNI, I., BECK, C.S., POTTS, R.C. CREE, LA. and ILIAS, N.I. Blood flow velocity in cutancus lesions of leprosy. Int. J. Lepr. 56(1988)394-400.
3. BARTEL, P.R., BAKER, M.K., CAMBRINK, P., ROBINSON, E. and VAN DER MAYDEN, C.H. Auditory brainstem evoked potentials in leprosy. S. Afr. Med. J. 73(1988)593-596.
4. BENEDICK, P.J. and GLOVER, J.L. Vertebrobasilar insufficiency: evaluation by quantitative duplex flow measurement. J. Vase. Surg. 5(1987)594-600.
5. BENEDICK, P.J. and JACKSON, V.P. Evaluation of the vertebral arteries with duplex sonography. J. Vase. Surg. 3(1986)523-530.
6. CANDIA, A. D. and MARIANA, A. Studies of cochleovestibular function in patients with leprosy. Rev. Audiol. Pract. 1(1965)7-9.
7. CHOPRA, J.S., KAUR, S., MURTHY, J.M. and KUMAR, B. Vascular changes in leprosy and its role in the pathogenesis of leprous neuritis. Lepr. India 53(1981)443-453.
8. DEBI, B.P., MOHANTI, H.C.TRIPATHY, N., TOMPE, D.B. and SARANGI, B.K. Artériographie pattern of plantar ulcers in lepromatous leprosy-study of 20 cases. Lepr. India 52(1980)429-432.
9. Dix, M. and HOOD, J. Vertigo Tests of Vestibular Function. New York: John Wiley and Sons Ltd., 1984, pp. 55-90.
10. EL-ARINI, F.G., SHEETA, N.A. and ABOU ZEID, S.A. Eighth cranial nerve affection in leprosy. Int. J. Lepr. 38(1970)164-169.
11. KATOCH, K., RAMU, G., SENGUPTA, U. and BHARADWAJ, V.P. Central nervous involvement in leprosy. Indian J. Lepr. 56(1984)813-818.
12. KYRIAKIDIS, M.K., NOUTSIS, C.G., ROBINSON-KYRIAKIDIS, C.A. and VENETSIANOS, P.J. Autonomic neuropathy in leprosy. Int. J. Lepr. 51(1983)331-335.
13. LATIF, S. The effect of certain skin diseases on the ear, nose and throat, M.Ch. degree thesis, Alexandria University, Egypt, 1967.
14. MIYASAKI, M. and KATO, K. Measurement of cerebral blood flow by ultrasonic Doppler technique. Jpn. Circ. J. 29(1965)375-382.
15. RAMACHANDRAN, A. and NEELAN, P.N. Autonomic neuropathy in leprosy. Indian J. Lepr. 59(1987)405-413.
16. ROCK, E.H. Vascular dizziness and transcranial Doppler ultrasonography. Ann. Otol. Rhinol. Laryngol. 98(1989)1-23.
17. SINGH, T.R., AGRAWAL, S.K., BAJAJ, A.K. and SINGH, M.M. Evaluation of audiovestibular status in leprosy. Indian J. Lepr. 56(1984)24-29.
18. USMANOV, R. Bone conduction of sounds in leprosy patients. (Abstract) Int. J. Lepr. 33(1965)252.
1. M.D., Associate Professor., Departmentof Otolaryngology, Medical Faculty, Firat University,Elazig, Turkey.
2. M.D., Assistant Professor., Departmentof Otolaryngology, Medical Faculty, Firat University,Elazig, Turkey.
3. M.D., Research Fellow., Audiology Technician, Departmentof Otolaryngology, Medical Faculty, Firat University,Elazig, Turkey.
4. Audiology Technician, Departmentof Otolaryngology, Medical Faculty, Firat University,Elazig, Turkey.
Received for publication on 12 July 1994.
Accepted for publication in revised form on 27 September 1994.
Reprint requests to Dr. Koyuncu, Department of Otolaryngology, Ondokuzmayis University Medical School, Samsun, Turkey.