- Volume 63 , Number 1
- Page: 123–32
News and notes
This department furnishes information concerning institutions, organizations, and individuals engaged in work on leprosy and other mycobacterial diseases, and makes note of scientific meetings and other matters of interest.
Brazil. Epidemiology Congresses to be held in April. From 24 to 28 of April 1995 the III Brazilian Congress, the II Ibero-American Congress and the I Latin-American Congress of Epidemiology will be held jointly in Salvador, Bahia, Brazil. This event is sponsored by the Brazilian Association of Graduate in Public Health (ABRASCO), by the Ibero-American Society of Epidemiology (SIAE), and by the Latin-American Association of Social Medicine (ALAMES).
The main theme of the meeting will be: "Epidemiology and the search for equity in health." The event will assemble epidemiologists and other health professionals to promote the interchange of knowledge, experiences and practices to foster the scientific development of the discipline and to define strategics aimed at transforming the living conditions of our populations.
Concurrently there will be an exhibit on technology in epidemiology (EPITEC) to show the development and use of technologies in collective health.
The program of the Congress includes conferences, round tables, as well as panels, coordinated communications and poster sessions. The conferences will be planned on: Epidemiology and equity in health; living conditions and health in the context of current socioeconomic changes in Latin America; violence and citizenship, toward a new life ethic; life and health in the cities.
The round tables will be on: The impact of social and economical policies on the epidemiologic profiles; inequalities in health; methodological advances in epidemiology, epidemiology and health services management; epidemiologic research in Ibero-America.
On April 24 and 25, prior to the Congress, mini-courses will be offered on: Survival analysis; confounding in epidemiology and statistics; sampling techniques; geoprocessing in epidemiological research; epidemiology in the evaluation of health services; qualitative methods in epidemiology; casecontrol studies; intervention studies; occupational epidemiology; work and the healthdisease process; bases of social epidemiology; rapid assessment techniques; molecular biology techniques for epidemiologic research; epidemiologic methods in reproductive health; epidemiologic methods in nutrition; epidemiologic methods in oral health; epidemiologic methods in the study of drug use and consumption; epidemiologic surveillance methods.
Workshops: Epidemiological information for decision making at the local level; National training programs in epidemiology health services; Use of epidemiologic criteria for allocation of health resources; Health surveillance: Legislation and organizational models; Perspective in use of epidemiologic methods in occupational health research.
Product lines and services to be presented at EPITEC:
Knowing the health conditions. Products and services for screening or studies aimed at assessing community health profiles. Data management and analysis. Resources (hardware, software, field data management techniques, etc.) for data management, processing and analysis in epidemiological research and surveillance.
Quality and management in the health services. Health information and informatic studies on quality of health care; information systems applied to financial and administrative and health planning; development of human resources in epidemiology.
Drugs and therapies. Drugs and therapies used in the fight against endemic infectious and chronic-degenerative diseases.
Hunger. Studies and actions conducted by nongovernmental organizations; products used in supplementary nutrition programs, studies and actions by federal, state, provincial and municipal governments.
Teaching health. Videos and other audiovisual resources; software; institutional offering (courses, training, etc.).
Institutional marketing. Space reserved for the use of teaching and research institutions in promoting their institutional marketing.
For further information: Congresso de Epidemiología-INTERLINK, Consultoria & Eventos Ltd. Av. Princesa Isabel, 573-B, Barra Avenida CEP 40.130.030, Salvador, Bahia-BRASIL., Phone: (55-71)247-2727/ 235-2284; Fax: (55-71)245-5633, E-mail: INTERNET- epidemio@sunrnp.ufba.br.
China. ILEP members fund Chinese shoe factory. In cooperation with the Chinese Government, Damien Foundation Belgium (DFB) and Sasakawa Memorial Health Foundation (SJ) have equipped a factory 200 km from Huan in Hunan Province.
The Chinese National Leprosy Program has estimated that a total of 70,000 patients would benefit from adapted footwear. Calculating each patient to need three pairs of shoes per year the project has planned a production capacity of 210,000 per year.
A shoe factory with an existing work force, over 100 employees and family members, has signed a 10-year agreement with the government to produce the required number of shoes.
The production line donated by the Belgian government through DFB is already in place and should be ready to start production by the end of 1994. A similar production line, donated by SJ, is currently being installed. With lines in place the factory will have a potential capacity of 1,000,000 pairs of shoes per year. This will allow the manufacture of shoes for commercial sale.
The material and labor cost of producing the footwear will in part be met by a $100,000 fund established by SJ to be provided over 5 years. This will pay for the production of 5000 pairs of shoes per year with a cost of $4 per pair. Further production costs will be subsidized by the government and by the commercial sale of ordinary footwear. The government also intends those patients who can afford it to pay at least part of the cost of their footwear.
Jean Watson, Consultant Physiotherapist for TLMI, will be advising on different materials; the equipment modifications needed to make appropriate footwear for leprosy patients; and the question of acceptable design. A period of experimentation will be necessary during which the employees will be trained in the production of adequate footwear for leprosy patients. -ilep flash 4/94(1994)p. 4
France. Diplôme Universitaire de Léprologie, 1994-1995 . Un enseignement théorique et pratique de léprologie est organise de janvier à mars 1995, à la Faculté de Médecine de Lariboisière/St-Louis sous la direction du Pr Louis Dubertret.
Peuvent s'inscrire les Docteurs en Médecine français, les étrangers pourvus du diplôme français de Doctorat d'Université (ou possédant un diplôme médical leur permettant d'exercer la médecine dans leur pays d'origine), les Internes en Médecine des CHR et les étudiants des UER médicales ayant validé leur stage pratique (le Certificat ne leur sera délivré officiellement que lorsqu'ils auront acquis le diplôme de Docteur en Médecine).
Renseignements: Pr Flageul (Service du Pr Dubertret) Hôpital St-Louis, 1, av. C-Vellefaux, 75475 Paris Cedex 10. Tél.: 42.49.98.16.
Germany. First European Conference on Tropical Medicine. We have received the following invitation from Prof. Dr. Manfred Dietrich, Conference Chairman, relative to the Conference to be held 22-26 October 1995 in Hamburg, Germany:
"You are cordially invited to come to Hamburg/Germany for the European Conference on Tropical Medicine. For the first time, the European Societies of Tropical Medicine have decided to arrange a European scientific Conference on Tropical Medicine. Although it is called a European Conference, one of the conference aims is to strengthen the links with colleagues from the tropical world. Therefore, as many colleagues as possible from tropical areas, especially Africa but also from South America and Asia, will be invited. The organizers hope that this conference will pave the way for further collaboration among the Europeans working in the field of tropical medicine and strengthen the collaboration between the scientists in European countries and those in tropical areas. It is not intended to interfere with individual interests of the national societies of tropical medicine.
"The conference will provide a forum for all disciplines of tropical medicine. Scientists in the laboratory and those in the field will meet together and exchange their views on common problems. As you can see from the proposed topics of the conference, there will be a variety of symposia and workshops on basic research, applied research, diagnostics, and treatment of tropical diseases. Field studies, problems of health in the tropics, of refugees and displaced persons, problems of nutrition and continuing education will also be included.
"The organizers are looking forward to your participation and will do their best to achieve a high scientific level while at the same time providing a convivial atmosphere."
Publication of invitation program: February 1995; abstracts must be submitted by 30 June 1995; authors will be informed by 8 September 1995; publication of final program: October 1995.
Conference Secretariat TROP '95: M. Rieger and C. Kuchenbuch, % CCH Congress Organization, Jungiusstrassc 13, P. O. Box 30 24 80, D-20355 Hamburg, Germany. Tel: 49(0)40-35 69 22 45; Fax: 49(0)40-35 69 23 43.
Conference Chairman: Prof.Dr. M. Dietrich, Bernhard-Nocht Institute for Tropical Medicine, Bernhard-Nocht-Stra.ssc 74, D-20359 Hamburg, Germany. Tel: 49(0)4031 18 23 90/1; Fax: 49(0)40-31 18 23 94; Telex: 2 163 853 trop d.
India. CLT&RI research project. "Impact of MDT on prevalence, new case detection and grade II deformities among new cases in districts completed 6 years or more of implementation and future projections.
"This new project was taken up and completed in 1993-94. Under the project the behaviour of certain epidemiological indicators of 4 districts of Andhra pradesh which have completed more than 6 years of MDT implementation has been studied. Relevant data have been collected from the districts of Srikakulam, Visakhapatnam, Chittoor and West Godavari for the post-MDT period 1983-84 to 1992-93. These districts covered a population of about 13 millions (estimated). A total of 100107 leprosy cases where detected during the above period and 133890 cases were discharged as RFT. Various indicators such as coverage of active case detection methods, period prevalence rate, point prevalence rate, new case detection rate etc. were generated using estimated population. Proportion of MB cases, child cases and deformity cases (Grade II and above) among new cases were also calculated and analysed.
"Coverage of active case detection work by total population survey varied markedly over time between the districts and in between the districts. Prevalence rates declined markedly during the first 5 years of implementation (% fall in point PR varying from 70.7 to 85.7 and in period PR varying from 56.7 to 80.4). The rate of fall after 5th year is found to be rather limited (% fall in point PR varying from 36.7 to 62.0 and in period PR varying from 13.6 to 48.3). The period PR may be a better indicator to get an idea of the load of work to be handled as point PR may go below new case detection rate (NCDR) (as in Visakapatnam) leading to possible erroneous inferences.
"The NCDR has in some years declined only marginally and shown slight increase in some districts for some years. NCDR in recent years are perhaps indicative of incidence rates as MB proportion among new cases has stabilized during this period. The proportion of deformed (Grade II) among new cases has not shown a consistent declining trend. It is seen that the NCDR is consistently higher in the case of adults as compared to that of children. It appears that while MDT has dramatically increased the rate of discharge through RFT as a result of shorter duration of treatment, it has had a very limited effect in interrupting transmission as witnessed by more or less constant NCDR and limited fall in prevalence rates in later years of implementation. Perhaps at a given point of time there are many more undetected cases in the community than on the register whose potential in maintaining transmission is not clearly known. With the mechanisms of transmission not well understood, it is obvious that a well organised programme with a potent intervention may not give an anticipated result. Further the result of the above analysis should make us very cautious in making projections for future in terms of eradication and/or elimination of leprosy by 2000 AD.
"(Investigators: 1. Dr. P. S. Rao, 2. Mr. G. Subramanian, 3. Mr. M. Subramanian and 4. Mr. E. Sathish Kumar.)" -Central Leprosy Teaching and Research Institute Annual Report 1993-1994, pp. 18-19
IAL 1993 MDT workshop. The Indian Association of Lcprologists (IAL) organized a two-day workshop at Madras during 20-21 July 1993. The purpose of this workshop was to assess the impact of the MDT program under the NLEP on the trend of leprosy. Reliable data sets from some districts and from some well-organized projects covered under MDT for 7 years or longer were presented at the workshop and discussed. Dr. M.D. Gupte, Officer-in-charge, CJIL Field Unit, Avadi, Madras, was the convenor of the workshop. Twenty-nine invitees from governmental and nongovernmental organizations working in NLEP participated in the workshop and ten other invitees had communicated their inability to attend the workshop.
The workshop was inaugurated by Mr. Justice Krishnaswamy Reddy. Data from Visakhapatnam and Chittoor (Andhra Pradesh), North Arcot and Dharmapuri (Tamil Nadu) districts as well as from special areas like Gudiyatham Taluk (SLRTC-Karigiri), CLTRI Field area, CJIL Field Unit, Gandhi Memorial Leprosy Foundation, DANLEP, Damien Foundation, LEPRA and The Leprosy Mission were presented and discussed. In addition, observations on MDT in Tamil Nadu, Baroda and Andhra Pradesh were also presented and discussed. There were also three special presentations: The problem of disabilities in MDT districts (Dr. H. Srinviasan), Criteria for handing over leprosy control work in The Leprosy Mission field areas to the government for integration (Dr. C. S. Walter), MDT and urban leprosy (Dr. J. O. Simon) to highlight certain special topics. Observations made during the workshop are given below.
MDT campaigns used to get introduced in a particular district in a particular year, say 1983, and it generally took 2 to 6 years to bring the entire district under MDT campaign. It would therefore be inappropriate to compare various parameters like prevalence and new case detection for, say, 1983 against 1990 to assess MDT impact, when total MDT coverage for the district was achieved only during 1989.
A steep decline in prevalence rates following introduction of MDT was universally observed. However, only about 30% of the known cases were discharged as cured by MDT and the remaining 70% cases had been discharged mostly at the stage of screening.
It was also noticed that, generally, during the initial 1 to 2 years of an M DT campaign, intensive case detection activities were taken up and there was also a rise in the number of voluntarily reporting cases, resulting in a sudden spurt in the new-case detection rate. During the subsequent phases of the campaign, there was more emphasis on case holding. It is thus highly inappropriate to make a simple comparison of new-case detection rates in the year of MDT introduction against the figure 7 years later. One should look for trend over a few years, than compare at two points of time.
Depending on the operational modalities adopted from time to time, there were fluctuations in the number of new cases detected and the proportions detected by various methods. In this connection, midstream changes in diagnostic criteria and treatment policies is one other important variable. Hence, it would not be proper to consider registered case detection and prevalence figures without taking note of these "correction factors" in the program. Some factors such as targets, and continuation of incentives to staff members are likely to influence substantially the quality of data being collected. The absence of a gold standard or objective diagnosis criteria, for early leprosy in particular, act as confounding factors at all the stages of the MDT campaign.
In spite of the difficulties listed above, consistent patterns were observed in several endemic districts under the MDT campaign. There was a definite and steep decline in prevalence, almost to the level of 10% of the original prevalence level. However, it was getting somewhat stabilized at the level of 1 per 1000. There was no apparent change in the new detection rate, although the profile of new cases showed changes. There was a significant increase in the proportion of child cases among the new cases. To a great extent, this was due to the increasing proportion of children being examined. There was a consistent decline in proportion of new cases with disabilities and an increase in the proportion of monolcsion cases. Paradoxically, the MB proportion was remaining somewhat constant.
A disturbing feature noticed was the big gap in the recorded prevalence and estimated prevalence, even after years of MDT implementation wherever sample surveys were undertaken, or where intensive case detection campaigns had been carried out. A large proportion of cases detected during these surveys are again cases of "early" leprosy which lead to debates on sensitivity and specificity of diagnosis. -Indian J. Lepr. 66(1994)411-412
Industrial participation in leprosy control.
Bombay Leprosy Project (BLP) celebrated its 18th anniversary on 6 October 1994 at Lccla Moolgaokar Leprosy Ward Agripada, Bombay Central, Bombay. On this occasion Prof. A. R. K. Pillai, President of the Indian Leprosy Foundation (ILEF), inaugurated the newer drug combination trial. On this occasion, he also congratulated the workers' union of Mahindra & Mahindra Company, Bombay, for their generous donation toward the cause of leprosy, especially chemotherapy trials. He also complimented BLP for undertaking a newer drug combination trial with ofloxacin, minocycline and rifampin to reduce the duration and offer cure to reach the goal of elimination of leprosy by 2000 A.D. Dr. C. R. Revankar, BLP Deputy Director, said that the current MDT and newer drugs are possibly the only hope to reach the elimination of leprosy. The government of India is making all out efforts to bring the whole of India under the MDT Program. However, research should continue in the field of chemotherapy to try out newer drug combinations to bring down the cost of treatment, duration and improved compliance of leprosy patients. Dr. V. V. Pai, Asst. Director, welcomed the guests and Dr. (Mrs.) R. S. Taranekar proposed a vote of thanks.
Karigiri staff news. The Karigiri Family welcomed the following new staff members: Mrs. Caroline Franklin as Nursing Superintendent on 30 September 1994.
Dr. Alexander Thomas as Physician with the Branch of Medicine on 3 September 1994.
Dr. (Mrs.) Rebecca Thomas as Ophthalmologist on 3 September 1994.
Dr. J. P. Anbarasu as Project Coordinator under DISLEP Project with the Branch of Surgery on 6 June 1994.
Mr. Jackson Samuel as Junior Programmer with the Data Processing Unit on 1 August 1994.
Dr. A. Sundaravaradan as Medical Officer with the Branch of Epidemiology and Leprosy Control on 21 September 1994.
Dr. Renu Jacob as Medical Officer with the Branch of Laboratories on 22 September 1994.
Mrs. Rebecca Vargheese as Master Tutor with Orthopaedic Appliance Unit on 8 August 1994.
Mrs. Valsa Augustine, Hon. Assistant Public Relations Officer, joined the Department as a regular staff on 15 June 1994.-From Karigiri Bulletin 22(1994)
Low Cost Disability Management Project in Bombay. The 125th Gandhi Jayanti provided the opportune time for the birth of an imaginative and need-based project "Low Cost Disability Management" in Bombay.
Mr. R. Narasimhan, Chief Guest and Senior Superintendent, Vocational Rehabilitation Centre (VRC) for Handicapped, Bombay, inaugurated the "Low Cost Disability Management" (LCDM) project in Bombay on the 125th birth anniversary of Mahatma Gandhi at the Bombay Leprosy Project (BLP) ornee, and said that services to leprosy patients should be integrated with those offered to other handicapped as is practised in VRC.
LCDM is a partnership project jointly managed by the BLP and the Indian Leprosy Foundation (ILEF). BLP will look after the medical component while ILEF will take care of the social and financial components. LCDM is a frontier project with futuristic vision. It aims at prevention, care and management of disabilities arising out of leprosy and provide scientific model for national adoption.
Dr. R. Ganapati, Director of BLP, said that BLP has two decades of experience in leprosy work. It has to its credit some disability management programs. Techniques such as prefabricated splints, grip aids for hand deformities as well as POP for foot deformities had been field tested by BLP extensively in Prakasam and Kurnool districts of A.P. with resounding success.
Prof. A. R. K. Pillai, ILEF President, said that Gandhi Jayanti offers an excellent opportunity to emulate the ideals for which Gandhiji lived and died. On the 125th birth anniversary of Mahatma Gandhi, Low Cost Disability Management is launched as a joint pilot project, covering Bharat Nagar Slum in East Bandra and Kalyan Block in Thane District initially. About 500 disabled persons will benefit directly.
Mr. S. Kingsley Physiotherapy Technician, welcomed the gathering and Dr. C. R. Revankar, BLP Deputy Director, proposed a vote of thanks.
New Director of Gandhi Memorial Leprosy Foundation (GMLF). Upon the retirement of Shri S. P. Tare, Shri D. S. Wele, who was GMLF Asst. Director (Health Education) until his retirement 2 years ago, was appointed as Honorary Director of GMLF on 1 July 1994-Kusht Vinashak 16 No. 7 & 8(1994)32
Schieffelin course schedule for 1995. The following courses will be offered by the Schieffelin Leprosy Research and Training Center, Karigiri, in 1995:
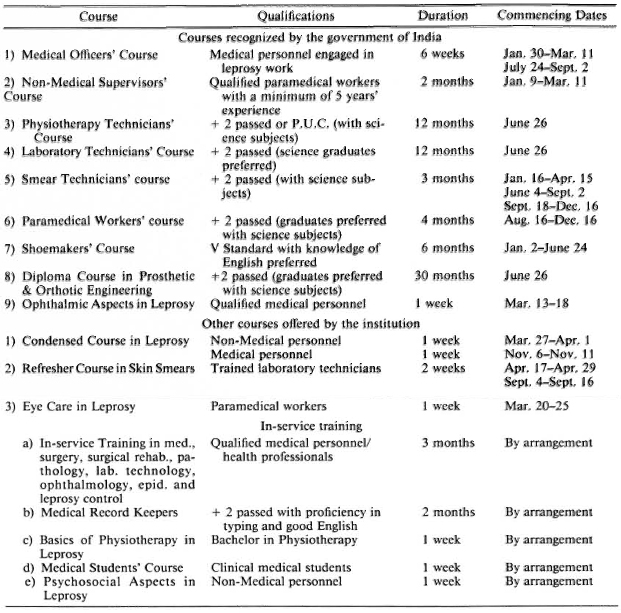
For details contact: Director/Head, Branch of Training/Training Officer, SLR and T Center, Karigiri 632 106, N.A.A. Disc, Tamil Nadu, South India (FAX = 91416-26759).-Materials from Sr. P. S. S. Sundar Rao.
Tare gives 1994 Erwin Stindl Memorial Oration. Shri S. P. Tare, Director, Gandhi Memorial Leprosy Foundation, gave the 1994 Erwin Stindl Memorial Oration entitled "Health Education in Leprosy." Following is the foreword by Hermann Kober, Vice-President, German Leprosy Relief Association:
"For the 11th Erwin Stindl Memorial Oration, GRECALTES Training Center chose the topic 'Health Education in Leprosy.'
"Health Education, that means informing the public, the medical staff and the patient about leprosy, is indispensable for the final victory over leprosy.
"This is all the more true as we now have drugs available which can cure leprosy.
"We need health education also to fight against the taboo which exists in view of this disease. It is needed in order to reintegrate cured patients into society and to prevent leprosy becoming an endemic disease again.
"I express my thanks to Dr. Chaudhury, Director of GRECALTES Training Center, for choosing this important topic and also to Shri S. P. Tare of the Gandhi Memorial Leprosy Foundation for deliverying this oration."
[Ed. note: The oration was delivered 30 January 1994, and has been published. Copies of this and earlier orations may be purchased from GRECALTES, 23 Market Street, Calcutta 700087, India, the proceeds to be used for leprosy teaching and control on a charitable basis.]
Tare retires from GMLF. After 39 years of long association with the Gandhi Memorial Leprosy Foundation (GMLF), Shri S. P. Tare retired on 30 June 1994. Shri Tare joined GMLF in 1955 as a statistician and then worked in various capacities and finally took the charge of Directorship of GMLF in 1982. His forceful presentation of his clearly argued out views on voluntarism, health education and rehabilitation in leprosy were felt in many a conference, seminar and committee in this country and abroad.-Indian J. Lepr. 66(1994)415
World Bank support to India. On 21 July in Delhi, the Indian Minister of State for Health, Dr. C. Silvera, led a formal meeting to inaugurate World Bank support to the NLEP. Around 150 personalities of antilcprosy work in India, including the Representatives of ILEP Members, attended the meeting
The new impetus for MDT implementation provided by Bank funds were presented by Dr. B. N. Mittal, Head of the NLEP, as a milestone in the history of leprosy control in India. He also provided valuable up-to-date statistics on the current position in India and pointed out that 95% of the national leprosy load was concentrated in ten states headed by Uttar Pradesh and Bihar.
The Minister set the importance of MDT implementation in the context of leprosy as a disabling disease. He and other speakers spoke in terms of grasping the opportunity offered now to bring treatment by the year 2000 to all who need it.
During the discussion period chaired by Dr. S. K. Noordccn of WHO a variety of people made comments which betrayed a certain scepticism as regards the possibility in India of reaching the target of elimination of leprosy as a public health problem within 6 years. There were references both to the continuing high level of new cases even in areas which have been using MDT for some time, and the problems of disability due to leprosy.
There was, however, evident excitement at the acceleration of the NLEP and a determination to grasp the opportunity offered by MDT together with current financial and political support. Dr. Mittal closed by urging all to join together in bringing treatment to every person who needs it. -ilep flash 4/94(1994) p. 5
Japan. $50 million donated to global leprosy program. Mr. Sasakawa, Jr., announced at the International Conference on the Elimination of Leprosy that the Sasakawa Foundation (Japan Ship-Building Industries Federation) will give $50 million over the next 5 years to support the World Health Organization's Global Elimination of Leprosy Program.
The money will be channelled through the WHO who are setting up the "Sasakawa Leprosy Elimination Trust Fund." The fund will receive $ 10 million per year for a period of 5 years. The donation is to be used for the purchase of MDT drugs and allocation will be in response to requests to WHO from the governments of leprosy-endemic countries. Sasakawa Foundation's contribution will cover about one third of the global drug requirements estimated necessary by WHO for the achievement of their elimination target.-ilep flash 4/94(1994) p. 3
Nepal. Changing of Director of INF LCP. On 18 November 1994 Dr. Wim H. van Brakel became the new Director of the International Nepal Fellowship Leprosy Control Project (INF LCP). Dr. van Brakel replaces Dr. Jeanette Hyland, outgoing Director, who has plans for research and some periodic consultancy to the INF LCP.
Switzerland. Leprosy upgraded within WHO. The Director General of the World Health Organization, implementing his intention to make leprosy a "Special Program," has decided to establish, with effect from 1 December 1994, an Action Program for the Elimination of Leprosy (LEP). The main objective of the program is to eliminate leprosy as a public health problem by the year 2000. The program will have the following three components:
Country Support and Special Action Projects (CSP)-Dr. L. Lopez-Bravo
Monitoring and Evaluation of Elimination of Leprosy (MEE) -Dr. D. Daumerie
Capacity Building and Health Systems Research (CBH)-Dr. S. Nkinda
Dr. S. K. Noordeen will become the Director of LEP with responsibility for policy setting; scientific direction; co-ordination with other agencies; advocacy, budget finance and administration. The Leprosy Control unit in the Division of Control of Tropical Disease will be disestablished, also with effect from 1 December 1994. -ilep flash 5/94(1994) p. 2
WHO Chemotherapy of Leprosy; report of a WHO Study Group. This new WHO publication (Tech. Rep. Ser. 847) contains the following recommended chemotherapeutic regimens for leprosy:
"Multibacillary leprosy
"The WHO MDT regimen for multibacillary leprosy has been very successful and has been widely implemented as recommended. Most data on the effects of limiting therapy to a 24-month course (rather than continuing until skin smears are negative) are favorable. The Study Group therefore recommended that all multibacillary patients be given the standard WHO regimen for 24 months, since it considered that such a change was safe and would increase the use of the regimen under field conditions.
"The Study Group also recommended that there should be no changes in the composition or doses of drugs, or in the "rhythm" (i.e., frequency and pattern) of therapy. Although the various new bactericidal drugs now available may alter this situation in the future, the Study Group pointed out that clinical trials would be needed before these drugs could be employed in MDT regimens.
"For adults the recommended standard regimen for multibacillary leprosy is:
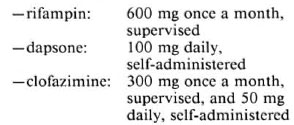
"Duration: 24 months
"The above regimen is suitable for the treatment of all categories of multibacillary patients except for those referred to in section 4.3. Cases of relapse should be confirmed by a referral center and the patients should be re-treated with the same regimen, since drug resistance is unlikely.
"Paucibacillary leprosy
"The 6-month WHO MDT regimen for paucibacillary leprosy has yielded excellent results wherever it has been appropriately used, and there is no convincing evidence to suggest that it should be extended beyond 6 months. The Study Group therefore recommended that the regimen be retained, with no changes in the duration or rhythm of therapy, or in the composition or doses of drugs.
"For adults the recommended standard regimen for paucibacillary leprosy is:
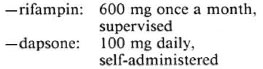
"Duration: 6 months
"If any patients relapse, they should be retreated with the same regimen, provided their disease is still paucibacillary. If, however, multibacillary leprosy is diagnosed at the time of relapse, treatment should be in accordance with the recommended regimen for that disease." -From pages 12 and 13 of the pamphlet
WHO Report of the Monitoring and Evaluation Meeting. The meeting was held in Orlando, Florida, U.S.A. on 28-29 August 1994. Major recommendations and conclusions as contained in the report are:
"The guidelines for conducting a leprosy elimination program review for program managers are very useful, because they focus mainly on monitoring operations with some epidemiological surveillance which can be carried out through sentinel surveys to assess progress as we approach the year 2000. The justification for a program review is to ensure we are on target and, if not, to take appropriate action. Most important is that the opportunity be given for all leprosy patients to be put on MDT."-From page 8 of the report (WHO/CTD/LEP/93.6)
U.K. Leprosy workers on the move. After 28 years with Aide aux Lepreux Emmaüs-Suisse (ALES), as General Secretary and, since 1990 as President, Walter Rosenfeld has announced that he will be retiring at the end of this year. He will continue working with his successor, Rolf Lehman, until June 1995.
ALES also has a new General Secretary, Rina Perolini, well known already to all ILEP Members, has formerly taken on the role of General Secretary from 14 December 1994.
Dr. H. Sudarshan, project director of the Karuna Trust Rural Health Project in Yelandur, was honored in Stockholm on 7 December 1994, when he received the alternative Nobel Peace Prize, the Right Livelihood Award, in recognition of his contribution to a process that secures the basic rights and fundamental needs of indigenous people and conserves their environment, enabling them to become more self-reliant and to contribute to the wider society.
Dr. P. Courtright has been appointed to the University of British Columbia in Vancouver. He is to develop an international ophthalmology unit for the university and hopes that work in ocular leprosy will become one of the specialties of the unit.
The President of CIOMAL, Mr. de Weck, will be retiring at the end of this year after more than 6 years with CIOMAL. His replacement is Maître Bruno. At the same time Dr. Millan has been appointed as the new medical advisor for CIOMAL.
At TLMI Alan Gray is joining the team in January as director of finance. Molly Clark, director of personnel, has retired.
Brent Ridgeway, director of finance and management at the International Union Against Tuberculosis, retired this year.
Dr. P. D. Samson is replacing Dr. Cairns Smith as TLMI's regional director for South- East Asia. Dr. Smith remains their medical advisor and continues to serve on the ILEP Medical Commission.
TLMI's regional director for Africa, Andrew Macintosh, is returning to Australia in February 1995. -ilep flash 5/94(1994)p. 3
U.S.A. 100 years at Carville. A hundred years of rich history made 30 November 1994 an occasion for celebration at the Gillis W. Long Hansen's Disease Center in Carville, Louisiana, USA.
During the centennial week there was plenty to see and do including historical lectures, films, photography displays, concerts, an "International Colloquium on the Future of Hansen's Disease Control and Research," religious commemorations and even a golf tournament and gala ball. In a special centennial program, approximately 700 people packed the auditorium to hear the memories and congratulations of prominent political and public health figures, people affected by Hansen's disease and representatives of voluntary agencies-including ILEP and ALM International. During the ceremony Dr. Robert Hastings, in the name of the International Journal of Leprosy, accepted the 1994 Damien Dutton Award. Congratulations to the IJL and to Carville for such important contributions through research, training and care to people with Hansen's disease during the last 100 years, -ilep flash 5/94(1994)p. 3
Leprosy statistics for 1993. In 1993, there were 187 new leprosy cases reported in the U.S.A. Seventy-five were diagnosed in California, 31 in Texas, 18 in Hawaii, 14 in New York City, and 11 in Florida. This level of new case detection is comparable to the levels seen prior to the increased influx of Indochinese refugees from 1978 to 1988.-MMWR 42 No. 53 (1994)
New leprosy cases in U.S. in 1994. There were 111 new leprosy cases reported to the Centers for Disease Control and Prevention for 1994. This compares to 187 for 1993. By way of comparison, there were 22,152 new tuberculosis cases reported in 1994 compared to 24,324 for 1993.-MMWR 43(1995)967