- Volume 62 , Number 3
- Page: 345–52
Extended schooling and good housing conditions are associated with reduced risk of leprosy in rural Malawi
ABSTRACT
Incidence rates of leprosy in Karonga District, northern Malawi, are analyzed by duration of schooling and housing conditions, controlling for age, sex, BCG scar and geographical zone of the household. There is a strong inverse relationship between the number of completed years of schooling and leprosy risk. Good housing conditions are also associated with a decreased risk of developing leprosy in this population. The effect of housing is seen most strongly in young people. It is hypothesized that schooling changes behavior and housing determines environment in ways which are relevant for the transmission of Mycobacterium leprae or for the appropriate priming of the immune system.RÉSUMÉ
Les taux d'incidence de la lèpre dans le District de Karonga, dans le Nord du Malawi, sont analysés en fonction de la durée de scolarisation et des conditions de logement, après controle pour l'âge, le sexe, la présence d'une cicatrice de BCG et la zone géographique d'habitation. Il y avait une forte relation inverse entre le nombre d'années de scolarisation et le risque de lèpre. De bonnes conditions de logement sont aussi associées avec une diminution du risque de développer la lèpre dans cette population. L'effet du logement est vu de la manière la plus forte chez les personnes jeunes. On émet l'hypothèse que la scolarisation modifie le comportement et que le logement joue sur l'environnement, de façon mais en rapport avec la transmission du Mycobacterium leprae ou avec l'activation adéquate du système immunitaire.RESUMEN
Se analizó la incidencia de lepra en el Distrito de Karonga, en Malawi del Norte, en función del tiempo escolar, de las condiciones de vida, de la edad, del sexo, de la cicatriz por BCG, y de la zona geográfica de los convivientes. Hubo una marcada correlación inversa entre el número de años escolares completados y el riesgo de adquirir la enfermedad. Las buenas condiciones habitacionales también estuvieron asociadas con una disminución en el riesgo de adquirir la enfermedad en esta población. El efecto de las condiciones habitacionales se observó más marcadamente entre la gente joven. Se hipotetiza que la mejoría en los hábitos de vida adquiridos durante la etapa escolar condiciona cambios en el medio ambiente que resultan determinantes tanto en la transmisión de Mycobacterium leprae como en la apropiada estimulación del sistema inmune.Epidemiological studies have shown consistently that age, sex, household contact and BCG vaccination are important determinants of leprosy risk (2,4,6,8,13). Among other factors suspected to influence the pattern of leprosy (1) are pregnancy and lactation (3), climatic conditions (5,15), and one or another aspect of the poverty complex. The latter hypothesis is frequently expressed, as by Jopling: "Bad housing conditions and inadequate food are important factors in the spread of leprosy, for domestic over-crowding, particularly at night, provides the ideal conditions for infection whether by droplets or by skin contact, and under-nourishment reduces cell-mediated immunity" (7). Despite a widespread belief in the association between leprosy and poverty, there have been few detailed studies of socioeconomic determinants and their implications. Since the confirmation of an association between leprosy and a particular aspect of poverty might provide important insights into the natural history of Mycobacterium leprae, or even provide a target for control programs, this remains an important issue (14).
This paper examines data on quality of housing and duration of schooling as risk factors for leprosy in Karonga District, northern Malawi. Since age, sex and the presence of a BCG scar have each been shown to be risk factors for leprosy in this population (12), results are adjusted for their effects where appropriate.
METHODS
The Lepra Evaluation Project, a longitudinal study of the epidemiology of leprosy, was initiated in Karonga District in 1979 (10). The design of the study required two total population surveys in order to relate leprosy found at the second survey with the information about suspected risk factors which had been collected at the first survey. After a pilot study in 1979, the first house-to-house survey was carried out from April 1980 until August 1984. The second survey was carried out from November 1985 until September 1989. It was combined with the intake phase of a vaccine trial against leprosy (and tuberculosis), the Karonga Prevention Trial. The methods of interviewing and examining for leprosy have been described in detail (9,10,11).
Approximately 112,000 individuals were interviewed and examined during the first survey. The fieldwork was household-based, thus information was collected relating to households and dwellings as well as to individuals themselves. Variables relevant to the analyses in this paper include those relating to the construction style of dwellings in which people slept, whether the dwellings were owned or rented, and the geographic location of the household. In addition to being examined for leprosy, all individuals were interviewed, including questions on present and past schooling. During the second survey, most attention was placed on examination for leprosy (and on recruitment into the vaccine trial). Interviews still included a question on schooling but no information was collected on dwellings.
For the purpose of these analyses a case of leprosy is a person in whom the overall diagnostic certainty is considered to be high (N and M group patients9). An incidence case is defined as a case of leprosy diagnosed in a person examined more than once, with an interval of at least 30 days between examinations, for whom there was no suspicion of clinical leprosy at the time of his or her first examination and who had no evidence of ever having received antileprosy treatment. In addition, patients who, on review of all of their records in 1992, were suspected with the benefit of hindsight to have had early leprosy at the first examination are excluded from the analysis (11).
All individuals were divided into four groups according to their duration of schooling at the time of last examination (see below): 1) those who had never attended school (excluding preschool children), 2) those who had attended primary school for 1-5 years, 3) those who had attended primary school for 6-8 years, and 4) those who had received or were receiving at least secondary education. Where there was a discrepancy between data collected at two different interviews the more plausible information was accepted. For example, if at the first interview a school name and standard were recorded but the individual later denied ever having gone to school, the first information was used for this analysis (see below). Information was disregarded (=considered missing) if two contradictory records appeared equally plausible. If age and schooling status were not consistent then records were checked for key-punch errors by looking at the original data.
People also were categorized according to the housing standards of their household - a "household" being a group of people recognizing one person as their head. Housing standards were defined in terms of the type or construction of dwellings-a dwelling being defined as any structure in which people slept. Four types of dwellings can be distinguished in Karonga District: 1) houses constructed with locally made burnt bricks, 2) houses made with sun-dried bricks or pounded mud, 3) houses constructed using wood or bamboo poles and interlaced twigs and rods for the walls which are later plastered with mud (wattle and daub dwellings), and 4) temporary shelters made out of grass, grain sacks, discarded oil drums and other material. If the household owned several dwellings, as is commonly the case, the best dwelling was used for the allocation to a group. Only dwellings owned by the head of the household or allocated with a job (for instance, civil servants who are given a government house as part of the conditions of service) are considered, because dwellings which are rented are likely to be used for only short periods of time and may not reflect the socioeconomic level of the household.
In order to control for the uneven distribution of leprosy within Karonga District, the area covered by the Lepra Evaluation Project has been divided into five "zones." These include a hilly area in the northwest (zone A), the lakeshore plain north of Karonga (zone B), Karonga town and neighboring villages (zone D), the stretch of land between the lake and the tar road going from Karonga to Mzuzu (zone E), and the hilly area west of this road (zone C). Individuals were assigned to one or another zone on the basis of the location of their household in the first survey.
Incidence rates of leprosy were calculated by age, sex, BCG scar status, amount of schooling and standard of housing. Individuals contributed time from their first examination until the first of the following: the date when first suspected to have leprosy, the date when recruited into the Karonga Prevention Trial (and vaccinated), or the date when last examined before 1 January 1990. Analysis is by contemporary age, not age at first examination, so that an individual who was 13 years of age when first examined in 1983 will have contributed 2 years at risk to the 10-14 age group and 3 years at risk to the 15-19 age group before his or her last examination in 1988. Poisson regression analysis (using EGRET) was carried out to estimate relative leprosy rates according to schooling and housing, controlling for age, sex, BCG scar, geographical zone of a household, duration of schooling, or standard of housing as appropriate.
RESULTS
Among a total of 83,439 individuals who fulfilled the criteria for inclusion in the analysis, there arose 427 incidence cases of leprosy (257 females and 170 males). Table 1 shows the numbers of individuals by the duration of their schooling and sex. Included in this table are preschool children and individuals with missing (discrepant) information. Nearly one third of the females never went to school but only one fifth of the males never attended school according to the information given. There is a corresponding excess of males over females attending 6-8 years of primary school, secondary school or tertiary education facilities. An attempt was made to validate these data by comparing responses at successive interviews. There were 13,718 individuals (5950 females and 7768 males) who at the first interview said they had 1-5 years of primary education and who were subsequently re-interviewed once. At the second interview, 25.2% (1505) of the females claimed that they had never attended school compared to only 9.1% (706) of the males.
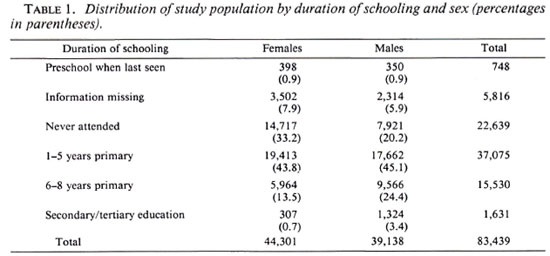
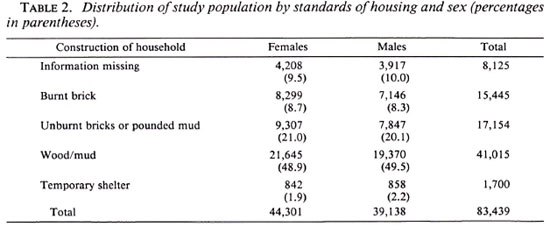
Table 2 shows the numbers of individuals by the best type of dwelling owned by the household and by sex during the first total population survey. Individuals renting their dwellings are categorized as "Information missing." There are no major differences by sex in this distribution.
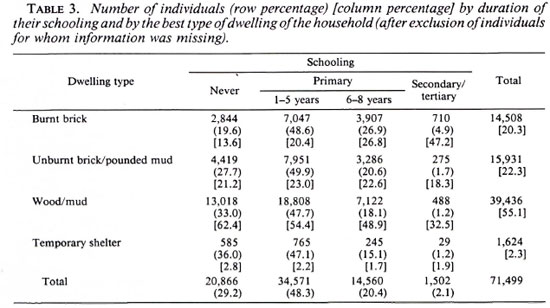
Individuals with missing information for duration of schooling or for standard of housing were omitted from subsequent analyses. This leaves 71,499 individuals, among whom there were 358 incident leprosy cases (218 females and 140 males). Table 3 shows the distribution of these individuals by duration of schooling and by the best type of dwelling owned by the household. There is a clear relationship between duration of schooling and type of dwelling. For example, 13.6% of people who never went to school belong to a household with at least one brick dwelling, while 47.3% of individuals who went to secondary school belong to such a household. Or, among members of a household with a brick dwelling, 19.6% never went to school, but among members of a household where a wattle and daub dwelling was the best dwelling 33% never went to school.
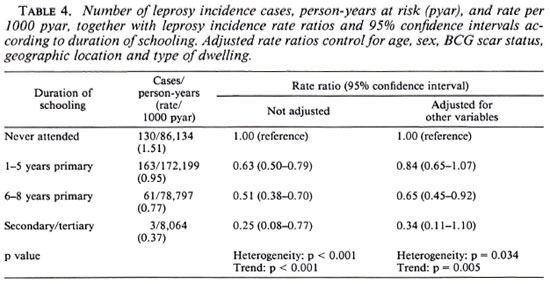
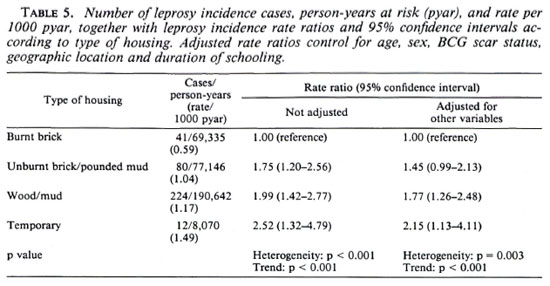
The average duration of follow up was approximately 5 years, giving 383,199 person-years of observation. Only one case occurred in the 0-4 years age group, which can by definition have had no schooling. This age group, therefore, was omitted from subsequent analyses. This left 357 incidence cases among 345,193 person-years of follow up. Tables 4 and 5 show the numbers of incidence cases, person-years at risk and unadjusted and adjusted rate ratios by duration of schooling and standard of housing, respectively. Table 4 shows that rate ratios decrease markedly with increasing duration of schooling, a relationship which is retained after controlling for age, sex, BCG scar status, standard of housing and geographic zone of the household. From Table 5, leprosy incidence rate ratios increase as the standard of housing falls from houses built of burnt bricks to temporary shelters. It thus appears that standard of housing and duration of schooling are each risk factors for leprosy in their own right.
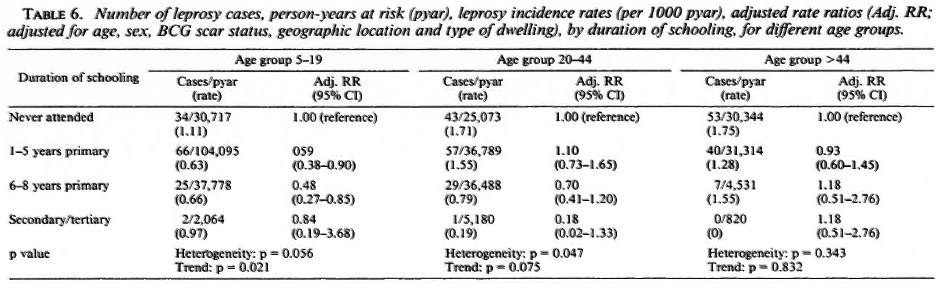
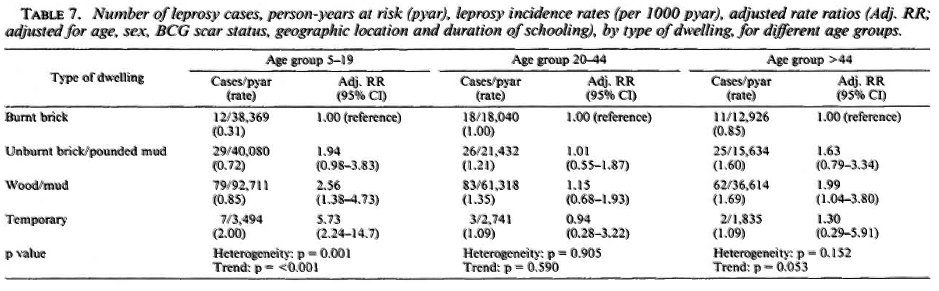
Tables 6 and 7 show the effects of duration of schooling and standard of housing, respectively, separately for age groups 6-19 years, 20-44 years and >44 years. It appears that the effects of schooling and housing are stronger among younger individuals (although the tests for interaction were not they actually saw during the first house-toformally statistically significant). The effect of schooling is present up to age 44 but not are bound to be less accurate because inthereafter, while the effect of housing is seen strongly in young people, not at all in younger adults, and equivocally in older people.
DISCUSSION
This paper shows that both poor standards of housing and lack of schooling are risk factors for the development of leprosy in this population. The dwelling data onwhich these analyses are based should be reliable, since the interviewers recorded what they actually saw during the first house-to-house survey. Data on duration of schooling are bound to be less accurate because interviewers had to rely on what they weretold. In children the wearing of a schooluniform was direct evidence of school attendance; in others a knowledge of impor-tant dates in English was a pointer toward past (or present) school attendance. Nev-ertheless, misclassifications as to the duration of schooling must be frequent, especially in older people. In particular, we have clear evidence that duration of schooling is underestimated in females. Misclassification thus may have masked a schooling effect among the older age group.
Parents in Malawi are not obliged to send their children to school. Primary school fees are nominal. However the fees and additional expenditure (e.g., for uniforms) can place a considerable burden on a poor family if there are several children attending primary school. Secondary school fees are substantial. If a child does well enough to be offered a place at a secondary school, even the extended family may have difficulties raising money for the fees, uniforms and (bus) fares to and from school. Tertiary education was free during the period of the study. For such reasons, school attendance is influenced not only by parental interest in education and the learning ability of the child but also by the socioeconomic level of the household. Until the 1960s, when many schools were built, schooling experience also was influenced by the distance to the nearest school. This, together with greater rates of misclassification of schooling status, may explain why there is no effect of schooling among older people. In addition, a considerable time has elapsed since this group were at school, so that any school-related influences may have disappeared by the time of this study. Indeed, it is likely that schooling in Africa 40 years ago had different implications from those which schooling has today.
The effect of poor housing on leprosy risk was even stronger than that of lack of schooling, but only among young people (Tables 6 and 7). It is important to note that housing is treated as a socioeconomic variable in this analysis insofar as we have allocated people to a group according to the best dwelling of the household and not according to the type of dwelling in which the person actually slept. Large households may own one burnt-brick house and several wattle and daub dwellings, in which some of the household members (e.g., the adolescent boys) would sleep. Thus, these findings cannot necessarily be taken as evidence that physical conditions of the home are relevant to leprosy risk, either through facilitating transmission of infection or through influencing the transition from infection to disease. However, the findings suggest that environmental factors-whatever they may be-are most important during childhood.
We explored the possibility that the association between leprosy incidence and low standard s of housing and schooling might be due, in part, to an association between multibacillary index cases and poorer or less well-educated households. However, controlling for the presence of index cases in the households at the time of the first survey had very little effect on the estimated rate ratios (a full analysis of the effects of contact with leprosy cases will be published separately).
These data show a strong direct or indirect influence of schooling and housing standards on leprosy risk in a rural African population. The results are consistent with the widespread impression of an association between leprosy and poverty and, in fact, provide one of the strongest demonstrations to date of this relationship. Just how the effects are mediated remains unclear. The age trends indicate that they relate to infection with M. leprae in early life, or to some earlyage exposure (e.g., with environmental mycobacteria) which influences the immune response to M. leprae. One possibility is that standards of hygiene are correlated with increasing duration of schooling and better standards of housing, and that these either decrease the chance that an individual will be infected with M. leprae or else lead to a better "priming" of the immune system. The formulation of more precise hypotheses for the findings presented in this paper await results of further analyses by variables related to personal behavior and individual contact.
Acknowledgment. The Lepra Evaluation Project is funded primarily by LEPRA (British Leprosy Relief Association) and ILEP (International Federation of Anti-Leprosy Organizations) with contributions from the WHO/UNDP/World Bank Special Programme for Research and Training in Tropical Diseases. The authors also thank the government of the Republic of Malawi for their interest in and support of the project, and the Malawi Ministry of Health for permission to publish the paper.
REFERENCES
1. Dharmendra. Role of non-genetic factors in susceptibility. Lepr. India 54(1982)721-782.
2. Doull, J. A., Guinto, R. S., Rodriguez, J. N. and Bancroft, H. The incidence of leprosy in Cordova and Talisay, Cebu, P.I. Int. J. Lepr. 10(1942)107-131.
3. Duncan, M. E., Melsom, R., Pearson, J. M. H. and Ridley, D. S. The association of pregnancy and leprosy. Lepr. Rev. 52(1981)245-262.
4. Fine, P. E. M. Leprosy: the epidemiology of a slow bacterium. Epidemiol. Rev. 4(1982)161-188.
5. Hunter, J. M. and Thomas, M. O. Hypothesis of leprosy, tuberculosis and urbanization in Africa. Soc. Sci. Med. 19(1984)27-57.
6. Irgens, L. M. Leprosy in Norway. Lepr. Rev. 51 Suppl. 1(1980)1-130.
7. Jopling, W. H. Handbook of Leprosy. 2nd cdn. London: Heinemann Medical Books Ltd., 1978, p. 4.
8. Noordeen, S. K. The epidemiology of leprosy. In: Leprosy. Hastings, R. C , ed. Edinburgh: Churchill Livingstone, 1985, pp. 15-30.
9. Ponnighaus, J. M., Fine, P. E. M. and Bliss, L. Certainty levels in the diagnosis of leprosy. Int. J. Lepr. 55(1987)454-462.
10. Ponnighaus, J. M., Fine, P. E. M., And Bliss, L., Sliney, I. J., Bradley, D. J. and Rees, R. J. W. The Lepra Evaluation Project (LEP), an epidemiological study of leprosy in northern Malawi. I. Methods. Lepr. Rev. 58(1987)359-375.
11. Ponnighaus, J. M., Fine, P. E. M., Sterne, J. A. C, Bliss, L., Malema, S. S. and Kileta, S. Incidence rates of leprosy in Karonga District, northern Malawi: patterns by age, sex, BCG status and classification. Int. J. Lepr. 61(1994)10-23.
12. Ponnighaus, J. M., Fine, P. E. M., Sterne, J. A. C, Wilson, R. J., Msosa, E., Gruer, P. J. K., Jenkins, P. A., Lucas, S. B., Liomba, G. and Bliss, L. BCG imparts greater protection against leprosy than against tuberculosis in northern Malawi. Lancet 339(1992)636-639.
13. Rao, P. S. S., Karat, A. B. A., Kaliaperumal, V. B. and Karat, S. Incidence of leprosy in Gudiyatham Taluk, South India. Indian J. Med. Res. 60(1972)97-105.
14. Sommerfelt, H., Irgens, L. M. and Christian,M. Geographical variations in the occurrence of leprosy: possible roles played by nutrition and some other environmental factors. Int. J. Lepr. 53(1985)524-532.
15. Stein, A. A. Lepra reaction and meteorotropism. Int. J. Lepr. 3(1935)137-152.
1. Dr. Med., D.T.P.H; Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
2. V.M.D., Ph.D; Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
3. Ph.D; Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
4. LEPRA Evaluation Project, P.O. Box 46, Chilumba, Malawi. Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
5. L. Bliss; Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
6. B.Sc, Communicable Disease Epidemiology Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WIE 7HT, U.K.
Current address for Dr. Ponnighaus: Universitats-Hautklinik, 66421 Homburg, Saar, Germany. Reprint requests to Dr. Fine.
Received for publication on 22 April 1994
Accepted for publication in revised form on 6 June 1994.