- Volume 62 , Number 2
- Page: 225–8
Autosensitization to connective tissue elements and endogenous adaptation hormones in mycobacterioses
ABSTRACT
The contribution of some adaptation hormones to the process regulating production of autoantibodies to collagen (Abe) and elastin (Abe) was studied in leprosy (37 patients) and tuberculosis (31 patients). In both mycobacterioses the Abe and Abe titers were increased and inversely correlated with endogenous Cortisol levels. In leprosy the antibody titers directly correlated with the triiodothyronine (T3) levels which were significantly higher than the values in healthy controls. A new approach to research for remedies and methods of preventing and curing autosensitization to connective tissue is suggested by combining medications according to individual endocrine and immune indices.RÉSUMÉ
La contribution de certaines hormones d'adaptation au processus réglant la production d'auto-anticorps visà-vis du collagène (Aac) et de l'clastine (Ace) a été étudiée dans la lèpre (37 patients) et la tuberculose (31 patients). Dans les deux maladies, les titres Aac et Ace étaient augmentés et inversement correlés aux taux de Cortisol endogène. Dans la lèpre, les titres d'anticorps étaient directement correlés avec les taux de triiodothyronine (T3), qui étaient significativement plus élevés que les valeurs observées chez les témoins en bonne santé. Une nouvelle approche à la recherche pour des remèdes et des méthodes de prévention et de traitement de l'autosensibilisation vis-à-vis du tissu conjonctif est suggérée en combinant des médicaments en fonction d'indices individuels endocrines et immunitaires.RESUMEN
Se estudió la contribución de algunas hormonas de adaptación al proceso de regulación de la producción de autoanticuerpos contra colágena (Abe) y clastina (Abe) en 37 pacientes con lepra y en 31 pacientes con tuberculosis. En ambas micobacteriosis, los títulos de Abe y de Abe estuvieron incrementados y correlacionaron de manera inversa con los niveles de cortisol endógeno. En la lepra, los títulos de anticuerpos correlacionaron en forma directa con los niveles de triyodotironina (T3), los cuales fueron significativamente más altos que los encontrados en los controles sanos. Se propone un nuevo enfoque para la investigación de remedios y métodos para la prevención y curación de la autosensibilización contra el tejido conectivo. Este enfoque considera la posible administración de medicamentos de acuerdo a los índices endocrino e inmunológico de cada individuo.In some mycobacterial diseases (leprosy, tuberculosis) strong autoimmunization aggravating clinical manifestations is observed. Thus, increased levels of antibodies to collagen (Abe) and clastin (Abe) are conducive to pneumosclerosis (13, l4) in pulmonary tuberculosis, and correlate to the most severe reactions such as erythema nodosum leprosum in leprosy (68 ). To what extent endogenous adaptation hormones are involved in autoimmune processes remains to be elucidated, and that was the aim of our work.
MATERIAL AND METHODS
Titers of Abe and Abe were estimated by the latex agglutination test (15). The levels of hypophyseal somatotrophic hormone (HSH), hydrocortisone (Cortisol), triiodothyronine (T3) and thyroxine (T4) were estimated in radioimmune assays (2, 3, 9, 10).
Thirty-seven patients with lepromatous leprosy (12 BL, 25 LL according to the Ridley-Joplingelassification) from 23 to 62 years old were included in the study. Among them were 17 females and 20 males.
Sixteen of the 37 patients had focal infiltrates on their skin. On biopsy a significant number of disrupted leprosy bacilli were found (active leprosy). In 21 patients only scarred lesions of residual leprosy were observed with no leprosy bacilli on biopsy (inactive leprosy).
All active leprosy patients were given multiple drug therapy (MDT) as recommended by the World Health Organization, and the patients with inactive leprosy received monotherapy with dapsone.
In the study 32 patients from 21 to 45 years old (15 females and 17 males) with pulmonary tuberculosis were included. The active stage of the disease was recorded in 19 patients (4 with disseminated tuberculosis in the phase of infiltration and degeneration, 10 with infiltrative and 5 with fibrocavernous tuberculosis in the phase of infiltration). All of the patients of this group discharged Mycobacterium tuberculosis with their sputum. In 13 patients the disease process was inactive (cirrhotic or focal tuberculosis in the consolidation phase with no tuberculosis bacilli in their sputum). All of the patients with pulmonary tuberculosis were given a combined chemotherapy irrespective of the phase of their disease.
Controls were 32 healthy persons.
Data obtained were analyzed using Spearman's rank correlation and Student's t test.
RESULTS AND DISCUSSION
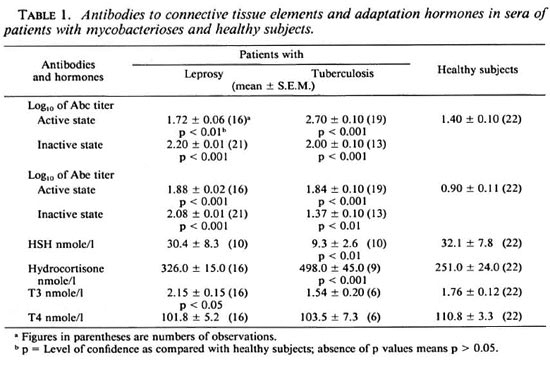
In active patients with leprosy and tuberculosis Abe and Abe titers were significantly increased (Table 1). In leprosy the Abe and Abe titers were increased in 50% and in 90% of the cases, respectively. In patients with tuberculosis Abe titers were more likely to be elevated than Abe titers. It is important that autoimmune manifestations remain in leprosy patients long after clinical regression has been achieved as judged by the maintenance of increased titers of Abe and Abe for many years. With a favorable course of pulmonary tuberculosis without excess fibrosis and emphysema of the lungs, antibody titers tended to fall toward normal during 4-6 months of therapy. In any case they were significantly lower than those at the peak of the disease (p < 0.01 for Abe and Abe) but they remained elevated as compared to the healthy controls. In both leprosy and tuberculosis patients high hydrocortisone and unchanged T4 levels were noted. HSH levels were significantly decreased in tuberculosis patients; in leprosy they were similar to those in healthy subjects. Increased levels of T3were observed only in leprosy patients. Ourinvestigation did not show any significantrelationship between the hormone levels andthe disease activity.
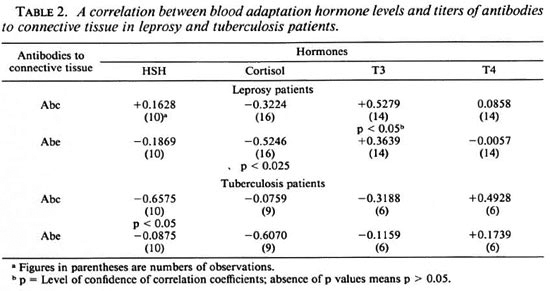
In both mycobacterioses a marked de-pendence of the antibody titers on hydro-cortisone, HSH and T3 levels was observedin a number of cases (Table 2).
Before proceeding to an assessment of thepathophysiological implications and signif-icance of these interrelationships, it is nec-essary to pay attention to the following,rather important, in our opinion, method-ological aspect.
The thing is that the two factors arestrongly correlated to each other on equalfooting, from the mathematical point of view (5). As applied to our data it would mean the following: the levels of the hormones have the same impact on the titers of the antibodies as the intensity of antibody production has on the levels of the hormones. Such a correlation can be demonstrated in experiments on intact laboratory animals (11). On the other hand, in chronic diseases such as leprosy and tuberculosis there are numerous metabolic, organic, psychophysiologic, etc., disturbances (7,12,13 ) which impact on the adaptation system and, hence, the production of the relevant hormones. Here the immunologic changes are only among the numerous factors affecting the adaptation system. It means that the coefficient of a correlation between the levels of the adaptation hormones and antibody titers in the patients with mycobacterial infections represents primarily the impact of the first factor on the second. Based on our data it can be stated with confidence that there is a unidirectional impact of adaptation hormones on the production of the antibodies toward connective tissue elements.
Abe titer was inversely correlated to the hydrocortisone level in both mycobacterioses. Since the hydrocortisone level had a tendency to increase (Table 1), it might be one of the factors preventing autosensitization to connective tissue both in leprosy and tuberculosis. The correlation between the Abe titers and the hydrocortisone level was not so obvious in our investigation.
A high negative correlation was noted between Abe production and the level of HSH in tuberculosis patients, but since blood levels of HSH are markedly low (Table 1), it is not likely that it plays a significant immunoregulatory role.
In leprosy patients the Abe and, to a lesser degree, the Abe titers were directly related to T3 levels. Taking into consideration increased blood levels of the antibodies studied and T3 hormone in leprosy, one may suggest a significant role of the latter in autosensitization to connective-tissue structures in this mycobacteriosis. In tuberculosis such a relationship was insignificant, probably because of the limited number of observations, and it needs to be studied further.
The correlations found may suggest a new approach to the search for remedies and methods of preventing and curing manifestations of autosensitization to connective tissue in mycobacterial diseases. There is no need to use only glucocorticoids, especially since the mycobacterioses under investigation are intrinsically related to deep disturbances of cell-mediated immunity (1,4) and may deteriorate because of the immunodepressive effect of the glucocorticoids. Production of antibodies toward connective tissue might be affected depending on the levels of endogenous thyroid hormones. It might be possible to combine medications according to individual endocrine and immune indices, hence decreasing the risk of side effects due to hormonotherapy.
Acknowledgment. The authors wish to express their gratitude to Mrs. V. Rezacva for technical assistance.
REFERENCES
1. AVERBAKH, M. M., GERGERT, V. Y. and LITVINOV, V. I. [Delayed type hypersensitivity and infection.] Moscow: Meditsina, 1974, p. 248.
2. BAUM, C. K.,TUDOR, R. and LANDON, J. A simple competitive protein binding assay for plasma Cortisol. Clin. Chim. Acta 55(1974)147-154.
3. DUNN, R. T. and FOSTER, L. B. Radioimmunoassay of thyroxine in unextracted serum by a single-antibody technique. Clin. Chem. 19(1973)1063-1070.
4. GODAL, T., MYKLESTAD, B., SAMUEL, D. R. and MYRVANG, B. Characterization of the cellular immune defect in lepromatous leprosy. Clin. Exp. Immunol. 9(1971)821-831.
5. GLUBER, E. V. and GENKIN, A. A. [Application of Nonparatnetric Statistical Criteria in Medico-biological Investigations.] Leningrad: Meditsina, 1973, p. 142.
6. KUZINA, Z. A. [Immunological Indices in the Patients with Lepromatous Leprosy and Their Dependence on the Severity of the Disease and Methods of Therapy.] Rostov-on-Don: Rostov Universiti Press, 1984, p. 176.
7. LOGINOV, V. K. and VISHNEVETSKY, F. E. [Combinative damage of kidneys and liver in the patients with lepromatous leprosy.] In: AktualnyeVoprosy Leprologii. Juscenko, A. A., ed. Astrakhan: Leprosy Research Institute Press, 1984, pp.98-101.
8. MEGHLAOUI, A., HERBAGE, D., Hue, A. and MONIER, J. C. Mice au point d'une technique immunoenzymatique (ELISA) pour la detection desanticorps au cours de la polyarthrite, rhumatoide,du lupus erythremateux dissemine et de Ia lepre.Ann. Immunol. 132(1981)287-305.
9. MOLINATTI, G. M. Radioimmunoassay of humangrowth hormone. J. Nucl. Biol. Med. 13(1969)25-34.
10. SEKADDE, C. B., SLAUNWHITE, W. R. and ACETO,T. Rapid radioimmunoassay of triiodothyronine.Clin. Chem. 19(1973)1016-1023.
11. SHKHINEK, E. Y., KORNEVA, E. A., SHTARK, E.,ACH, ZH., ABAVARI, K., SALAN, K. and FIOK, YA. [Glucocorticoid hormones and humoral immunity.] In: Regulatsia Immunnogo Ilomeostaza.Korneva, E. A., ed. Leningrad: Academy of Sciences of the USSR, 1982, pp. 113-114.
12. VELIKANOVA, L. P. and USHAKOV, G. K. [Borderline Nervous and Psychic Disturbances in Leprosy Patients.] Moscow: All-Union Institute for Medical Information, 1981, p. 9.
13. VINNICK, L. A. [Proteolytic enzymes and antigenity of connective tissue in tuberculosis and nontuberculosis diseases.] In: Reaktivnost Organismai Antigennost Soedinitelnoi Mani Pri Tuberkulosei Netuberkulesnih Zabolevanijah Legkih. Vinnick,L. A., ed. Saratov: Saratovsky Medical Institute,1986, pp. 5-54.
14. VINNICK, L. A. and GEROVITCH, L. M. [Activityof proteases and anti-connective tissue antibodylevels in lung diseases.] Terapevticheskiy Arhiv 3(1985)83-85.
15. VINNICK, L. A. and STRELTSOVA, E. N. [A methodof diagnosis of repaative processes in pulmonarytuberculosis.] In: I fobretatelstvo i Ratsionalifatsiav Meditsine. Demidov, B. S., ed. Moscow: RussianCentral I Central Institute of Tuberculosis, 1983, pp. 132-135.
1. M.D.; SeniorScientilic Worker, Head of Medical Radiology Laboratory, Leprosy Research Institute, GSP-7, Astrakhan 414000, Russia. Professor
2. M.D.; Astrakhan Medical Institute, Russia.
Received for publication on 2 February 1994;
Accepted for publication in revised form on 2 March 1994.