- Volume 62 , Number 1
- Page: 567–9
Disabilities among rural leprosy patients in Myanmar
In an effort to increase the utility of the JOURNAL in continuing medical education, in this section we welcome contributions dealing with practical problems in leprosy work. Submissions to this section will undergo minimal editorial changes and may well contain controversial points. Letters to the Editor pointing out other viewpoints are welcome.
Leprosy is a major health problem in Myanmar (formerly Burma). As of December 1990, 112,129 cases were registered for treatment throughout the country for a registered prevalence of 2.76 per 1000 population1. During the past decade, the registered leprosy cases have declined dramatically from a high of 240,000 in 1984 2 to 112,129 in 1990. This decline, if considered alone, masks the continued need for health care among disabled leprosy patients.
Since 1974, 144,000 leprosy cases have completed treatment and been discharged from the treatment program in Myanmar. Prior to multidrug therapy (MDT), only indeterminate and tuberculoid forms of leprosy were discharged from the treatment register. It was only after MDT that large numbers of cases were discharged. Some of these were suffering from disability at the time of discharge. It is well known that chemotherapeutic measures will never restore the function of the peripheral nerves once they have been damaged by the disease. Therefore, some discharged cases, though cured of leprosy, may still need medical care because of disabilities. Apart from the medical needs, some leprosy patients will, for the rest of their lives, suffer from physical, psychological and social problems as a consequence of having contracted leprosy. In addition to those with already established disabilities, some, who were free of disability at the time of discharge, also develop disability later as a result of residual anesthesia.
Understanding the scope of the disability problem among individuals who presently are suffering from leprosy, and also among those who once had leprosy, would facilitate the planning and implementation of appropriate measures aimed at helping disabled leprosy patients lead a productive life. The short duration of treatment needed with the present MDT regimen and the massive reduction in caseload drastically reduces the time previously spent for the delivery of drugs. Health care workers, especially those of the leprosy control program, now may have more time to care for these disabled leprosy patients.
Although estimates of the magnitude of the disability problem among registered cases or new leprosy cases have been made from time to time in order to assess the quality of the leprosy control services, the disability problem among all individuals who have had leprosy has never been studied in Myanmar. This study was undertaken to find out the magnitude of the disability problem among both leprosy patients currently under treatment and also among those who have been discharged.
MATERIALS AND METHODS
A cross-sectional survey was conducted in Hmawbi Township. This township was chosen because of its proximity to the city of Yangon and also because the records of old leprosy cases discharged from the treatment register could be traced back to each village for the past 15 years. At the time of the survey (May 1991), 180 cases were registered for treatment, and a total of 615 cases had been discharged, some treated with dapsone monotherapy and some with MDT. Out of a total of 96 villages having registered leprosy patients in the past and at present 17 villages were chosen by the investigator with priority given to villages with the highest number of known leprosy cases (cases still under treatment and those discharged combined). The total population of these 17 villages was 78,167. A total of 145 cases were reviewed out of 101 registered cases and 133 discharged cases residing in these 17 villages. Eighty-nine cases could not be reexamined because they were temporarily away from home at the time of the survey. Among these 89 cases, 84% were males and a review of treatment records revealed that only 5.62% of them had grade 2 disability.
The MDT regimen used in Myanmar is based on WHO guidelines3. After completing the recommended course of MDT, patients are released from treatment and put under surveillance. At the time of release from treatment, each case was removed from the treatment register and categorized as a discharged case. Prior to the introduction of MDT (during the days of dapsone monotherapy) lepromatous cases were treated for life, and indeterminate and tuberculoid leprosy cases were released from control only after having become inactive for 3 years and 2 years, respectively. Leprosy cases released from control under dapsone monotherapy also were included in the study. Patients were examined for disabilities using the disability grading formulated by WHO, a simple three-grade (0, 1 and 2) system4. Mantel-Haenszel Chi was used for statistical testing along with least square linear regression for the testing of trends.
RESULTS
Overall results of the 145 leprosy cases reviewed, 48 (33.1%, 95% CI = 25.45%40.75%) had disabilities, 29 of them (20% of the total) with grade 2 disability (Table 1). Grade 1 disability was found in 19 cases (13.1%). Sixty-seven patients were under treatment and 78 were discharged patients. Thirty of the 67 patients under treatment (44.8%, 95% CI = 32.9%-56.7%) had disabilities, 18 (26.9%) having grade 2 disabilities. Thus, 60% (18 of 30) of the dis-abled persons in this group had grade 2 disabilities. Of the 78 discharged patients,18 (23.1%, 95% CI = 13.7%-27.9%) haddisabilities, of whom 11 had grade 2 disabilities (14.1%). Thus, 61.1% of the disabled persons in this group had grade 2 disabilities.
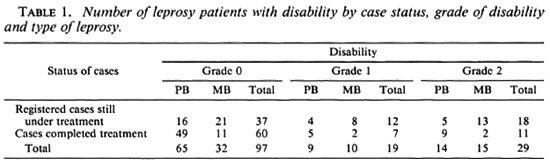
MB vs PB. Of the 88 paucibacillary (PB)cases, 23 (26.1%) had disabilities (grades 1and 2); of the 57 multibacillary (MB) cases,25 (43.9%) of them had disabilities. MBcases had significantly more disability thanPB cases (p = 0.028). Out of these 25 MBcases with disabilities, 15 had more severe (grade 2) disabilities (26.3% of the total) compared to the 14 PB cases (15.9% of thetotal). In terms of grade 2 disability, no significant difference was seen between PB andMB cases (p = 0.129).
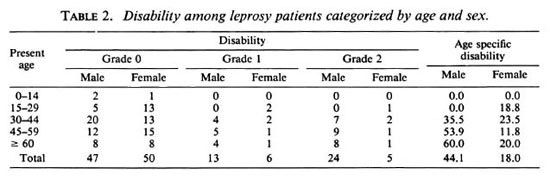
Age and gender. Table 2 shows that among the 84 male leprosy cases re-examined 13 (15.5%) of them had grade 1 disability and 24 (28.6%) had grade 2 disability. The overall disability rate among the males was 44.1% (95% CI = 33.4%-55.7%).Of the 61 female leprosy cases that were re-examined, 6 (9.8%) had grade 1 disabilityand 5 (8.2%) had grade 2 disability, respectively. The overall disability rate among females was 18.1% (95% CI = 8.4%-27.7%). In the 30-to-44 years of age category (both sexes), 15 (31.3%) had disabilities, of whom 11 (22.9%) were males and 4 (8.3%) were females. In the 45-to-59 years of age category, 16 (37.2%) had disabilities, of whom 14 (32.6%) were males and 2 (4.7%) were females. Among the 60 years and older age group, 14 (46.7%) had disabilities. Among the males, disability increases with age (b = 1.16, r = 0.957). This rising trend also was observed among females (b = 0.82, r = 0.633) but was not marked as in the males.
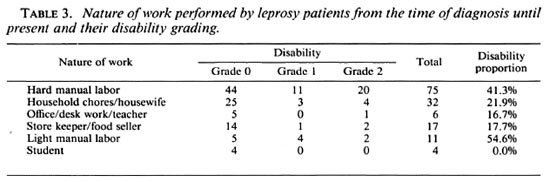
Occupation. In regard to occupation (Table 3), out of a total of 11 employed in light manual labor, 6 (54.6%) had disabilities (either grade 1 or grade 2) and among 75 hard manual laborers, 31 (41.3%) cases had disabilities. These proportions are not statistically different. The proportions with disabilities among patients giving job descriptions of household work/housewife, office work/desk work/teacher and store keeper/food seller are almost the same. The proportions of disability in hard manual laborers (31 among 75) are higher than those among all the other occupations combined (17 of 70, p = 0.066).
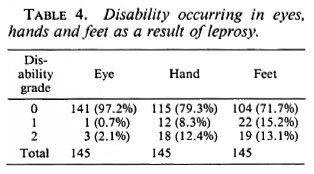
Location of disabilities. As seen in Table 4, out of 145 leprosy cases re-examined, 4 (2.1 %) had grade 2 disability in the eyes with their vision greatly impaired as a result of leprosy. Out of the 30 cases with disability of the hands, 18 (12.4% of the total) were grade 2 disability and 12 (8.3% of the total) grade 1. Of the 41 with disabilities of the feet, 19 were grade 2 (13.1% of the total) and 22 grade 1 (15.2% of the total).
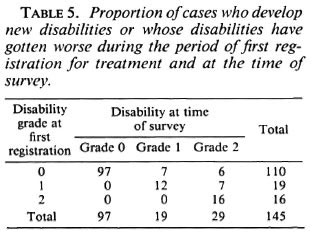
Disabilities after registration. As seen in Table 5, out of 19 cases with disability grade 1 at the time of first registration, 7 cases (36.8%) worsened and went on to develop grade 2 disability. Among 110 cases with no disability at the time of first registration, 13 cases (11.8%) developed new disabilities; 6 (5.5%) were grade 2 disabilities. Overall, in 20 leprosy cases (13.8%) new disabilities either developed or their old disabilities got worse during the period between their first registration and the time of the present reexamination.
DISCUSSION
The overall disability proportion among cases currently under treatment and those who have completed treatment was 33.1% (95% CI = 25.5%-40.8%) and grade 2 disability was seen in 20% (95% CI = 26.5%13.5%) of all cases. This shows the number of leprosy patients in the community having problems associated with disability to be quite high. Among the discharged leprosy cases, 23.1% were suffering from disabilities. Since more and more leprosy cases are expected to be discharged in the coming years, the rehabilitation program will have to reach out to such patients who would normally no longer be in contact with the leprosy control program on a regular basis. These discharged cases, even though they may have been successfully cured of leprosy bacteriologically, will still be in need of health care services because of their disabilities.
Although the overall disability proportion was found to be significantly higher in the MB patients, there was no significant difference in the more severe forms of grade 2 disability among PB and MB patients.
Males are seen to have a higher disability proportion compared to females (p < 0.003) but the reasons for this difference could not be satisfactorily explained in this study. Males also were more often observed to be suffering from grade 2 disability (p < 0.003). It could be that males are more involved in manual work.
Disability was observed to progress as age increased in males but this trend was observed only weakly among females. Further in-depth studies into the differences in disability patterns among males and females need to be done to understand more about this problem. Patients with an occupational history of light manual labor seem to be having more disability than those employed in sedentary work, such as household chores/housewife (p = 0.044) and store keeper/food seller (p = 0.046), indicating that the nature of the occupation may have prevented disability and that a change in occupation will have to be provided for some leprosy patients during rehabilitation. There were no differences in the disability proportions among the light manual laborers and hard manual laborers. This might be the result of a shift from hard manual labor to light manual labor after disability has developed.
Damage to the eyes was seen in 2.8% of all of the cases. The importance of early intervention in these cases needs to be stressed since such cases could become totally dependent upon society if not properly cared for during the early stages of the disease.
Out of all the cases reviewed, 13.8% were observed to have gotten worse with respect to their disability condition during the time between first registration for treatment and the time of this survey, indicating that proper education regarding care of their anesthetic hands and feet as well as rehabilitative measures are needed to prevent this shift. The majority of cases whose disabilities had gotten worse were in the category of grade 1 disability at the time of first registration (36.8%), which means that if this worsening of disability is to be avoided, preventive measures need to be started from the time of first treatment.
Acknowledgment. The authors would like to thankthe leprosy control workers from the Hmawbi LeprosyControl Project and those basic health workers fromthe Hmawbi Township Health Department for theirsupport in the conduct of this survey.
- Myo Thet Htoon, M.B., B.S.,
M. Med.Sc, M.P.H.
Epidemiologist
Leprosy Control Program
Department of Health
Yangon, Myanmar
- Zaw Win, M.B., B.S.
Team Leader
Hmawbi Leprosy Control Project
Yangon Division Health Department
Yangon, Myanmar
1. Leprosy Control Program. Annual Report of the Leprosy Control Program, 1984. Yangon, Myanmar: Department of Health, Ministry of Health, 1985.
2. Leprosy Control Program. Annual Report of the Leprosy Control Program, 1990. Yangon, Myanmar: Department of Health, Ministry of Health, 1991.126
3. WHO Expert Committee on Leprosy. Sixth report. Geneva: World Health Organization, 1988, p. 35. Tech. Rep. Ser. 768.
4. WHO Study Group. Chemotherapy of leprosy for control programmes. Geneva: World Health Organization, 1982, pp. 24-26. Tech. Rep. Ser. 675.