- Volume 61 , Number 4
- Page: 586–91
Altered calcium-binding ability of plasma proteins as the cause of hypocalcemia in lepromatous leprosy
ABSTRACT
This paper reports a study performed on 10 lepromatous leprosy outpatients and on the same number of age- and sex-matched contacts. All of the lepromatous patients were hypocalcemic, but plasma levels of ionized calcium and the acid-base status were normal. The average daily food intake assessed through a questionnaire revealed adequate nutrition of patients and controls. Plasma proteins and 1,25-dihydroxy vitamin D3 and intestinal absorption of calcium were discarded as the causes of the hypocalcemia. In vitro experiments designed to investigate the effect of hydrogen ion concentration on the equilibrium between calcium ion and proteins revealed that, at normal pH values, plasma proteins f rom lepromatous leprosy patients bind a smaller fraction of total plasma calcium than those f rom controls. This phenomenon produces a normal concentration of ionized calcium that determines a normal parathyroid status as indicated by the normal urinary excretion of hydroxyproline and plasma concentrations of alkaline phosphatase (total and bone isoenzyme) and tartrate-resistant acid phosphatase.RÉSUMÉ
Cet article relate une étude réalisée parmi 10 patients lépromateux externes et le même nombre de contacts appariés pour l'âge et le sexe. Tous les patients lépromateux étaient hypocalcémiques, mais les taux plasmatiques d'ions calcium et le statut acide-base étaient normaux. L'absorption quotidienne moyenne de nourriture évaluée à l'aide d'un questionnaire a montré une nutrition adéquate des patients et des témoins. On a écarté les protéines plasmatiques, la 1,25-dihydroxyvitamine D, et l'absorption intestinale du calcium comme causes de l'hypocalcémie. Des expérimentations in vitro réalisées pour analyser l'eflet de la concentration en ion hydrogène sur l'équilibre entre l'ion calcium et les protéines ont montré qu'à des valeurs normales du pH, les protéines plasmatiques provenant de patients lépromateux se lient à une part plus petite du calcium plasmatique total que celles provenant des témoins. Ce phénomène produit une concentration normale de calcium ionisé qui détermine un statut parathyroïdien normal comme l'indiquent l'excrétion urinaire normale d'hydroxyproline et les concentrations plasmatiques de phosphatase alkaline (totale et l'isoenzyme osseux) et de phosphatase acide résistant au tartrate.RESUMEN
Este trabajo reporta un estudio realizado en 10 pacientes lepromatosos ambulatorios y en 10 de sus contactos aparcados por edad y sexo. Todos los pacientes lepromatosos fueron hipocalcémicos pero los niveles plasmáticos de calcio ionizado y el estado ácido-base fueron normales. El consumo diario de alimentos, establecido a través de un cuestionario, fue adecuado tanto en los enfermos como en sus contactos. Las proteínas plasmáticas y la 1,25-dihidroxivitamina D3, así como la absorción intestinal de calcio, fueron descartadas como causas de la hipocalcemia. Los experimentos in vitro diseñados para investigar el efecto de la concentración del ion hidrógeno sobre el equilibrio entre el ion calcio y las proteínas, revelaron que a valores normales de pH las proteínas plasmáticas de los pacientes lepromatosos enlazan una menor fracción del calcio total que las proteínas plasmáticas de los controles. Este fenómeno produce una concentración normal de calcio ionizado que determina un estado paratiroideo normal, según se deduce de la excreción urinaria normal de hidroxiprolina y de las concentraciones en plasma de fosfatasa alcalina (la total y la isoenzima ósea) y de la fosfatasa acida resistente al tartrateLepromatous leprosy (LL) is characterized by an uncontrolled bacillary growth together with multiple and widespread lesions. The lepromatous form of the disease is important not only for the maintenance of the source of infection in the community but also as a cause of disabilities and a variety of sequelae as well as having systemic repercussions. In fact, LL is known to produce renal and hepatic involvement along with several biochemical alterations such as abnormal plasma levels of hormones, enzymes and minerals.
Low circulating calcium levels have often been found in LL (4,12,14,20,21,23) but little attention has been paid to the causes that may account for this abnormality. The present study was undertaken to determine the origin of the hypocalcemia found in LL patients.
PATIENTS AND METHODS
In a first approach, plasma calcium (25), albumin (5) and total proteins (7) concentrations were measured in plasma samples from 34 LL patients and from 36 age- and sex-matched, healthy, close contacts. The patient group consisted of 24 men and 10 women with a mean age of 55 ± 5.6 (S.D.) years. All of them were outpatients periodically attending the Leprosy Clinic for treatment and control. Twenty-three patients had active disease and seven of them had experienced type 2 reactions in the last 6 months. Six patients were newly diagnosed untreated cases; the rest of the patients were being treated with the following therapeutic regimens: dapsonc (DDS) 100 mg daily (N = 16), rifampin (RMP) 600 mg plus DDS 100 mg daily (N = 9), and multidrug therapy (MDT; DDS 100 mg/daily, clofazimine 50 mg daily, and RMP 600 mg + clofazimine 300 mg monthly, supervised (N = 3)). The mean duration of treatment was 13.2 ± 7.8 years. The patients had stable disease at the time of evaluation and were free of concomitant pathological disorders. Plasma samples were obtained at the Central Laboratory of the Hospital Provincial de Rosario and were drawn on occasion of routine laboratory screening.
In a second step, a smaller group of consenting individuals, 10 LL patients and 10 household contacts, volunteered to participate in an investigation dealing with the intestinal absorption of calcium. The LL group was composed of seven men and three women, mean age 48 ±1 1 years, who were under treatment with MDT (9) or DDS (1). The project was approved by the Ethics Committee of the Facultad de Ciencias Médicas, Universidad Nacional de Rosario.
After an overnight fast, blood was drawn with heparinized syringes; pH, pO2, pCO2 were determined with a radiometer. Plasma was saved to measure calcium (25), total proteins (7), albumin (5), alkaline phosphatase and its bone isoenzyme (18), tartrate-resistant acid phosphatase (2), creatinine (3) and 1,25-dihydroxyvitamin D3 (6). Ionized calcium was measured with a flow-through specific electrode (Orion Biomedical SS-20).
Urinary calcium (25), creatinine (3) and hydroxyproline (13) were measured on 24hr samples. The calculation of creatinine clearances was performed by the standard procedure.
Intestinal absorption of calcium was measured as indicated elsewhere (19). The results are expressed as percentage of test dose of calcium. Calcium intake was estimated by means of a questionnaire, recalling the intake during the last 7 days. Daily intake of nutrients was calculated with the aid of food composition tables. Calcium balances were estimated by the formula:
(Ca intake x % absorbed) = urinary Ca.
The dissociation of calcium protcinate complexes as a function of pH was investigated, adjusting the [H+ ] in the range 4 to 120 nM (pH 6.9 to 8.4) of two pools of sera (control and LL) with 1 M acetic acid. The protein-unbound calcium fraction was separated by ultrafiltration (17) and measured by atomic absorption spectrophotometry (25). The concentration of ultrafilterable calcium was expressed as percentage of total plasma calcium. The LL pool employed had 7.4 g/dL of total proteins, 5.3 g/dL of albumin, and 8.3 mg/dL of calcium; that of contacts had 7.1, 3.8 and 9.8, respectively.
Student's t test and regression analysis were employed for assessment of the data (24).
RESULTS
The findings obtained in the first part of the study (The Table) confirmed the presence of hypocalcemia in LL patients concurrent with significantly higher plasma proteins and albumin concentrations. Further study of a subset of 10 LL patients and their household contacts revealed, however, that plasma ionized calcium concentration and blood pH, pCO2 and bicarbonate were within normal values.
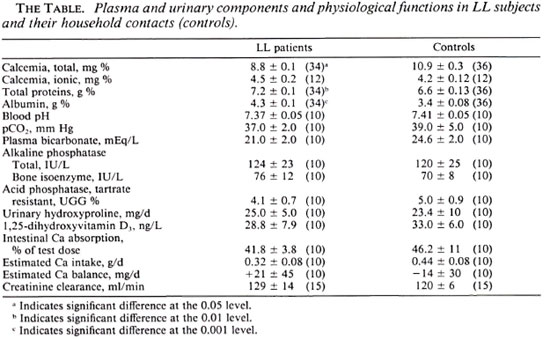
Investigation of food intake revealed a large variance of the data which was attributed to the wide range of social and cultural backgrounds of LL subjects and their household contacts. As expected, comparison of food intakes between the two groups yielded no statistical differences. Carbohydrates intake ranged from 157 g/d to 483 g/d, proteins from 32 g/d to 167 g/d and fat from 15 g/d to 166 g/d. Food intake averaged 2200 kcal/d with a range 985-3620 kcal/d. Only two patients and one contact would quality as undernourished according to their responses to the questionnaire. On the average, the intake of basic nutrients of LL patients and contacts (carbohydrates, proteins and fat) expressed as percentages of total kcalories/d were 51%, 16% and 33%, respectively, quite close to some dietary goals (22) (58%, 12% and 30%, respectively).
To address the question of whether or not malabsorption of calcium was related to hypocalcemia, the plasma levels of 1,25-dihydroxyvitamin D, and calcium absorption were measured. As shown in The Table, similar values were obtained from both groups and, therefore, chronic malabsorption and/or a disturbance of vitamin D3 metabolism was ruled out. In agreement, Kumar, et al. (10) have reported normal structure and function of the bowel of LL patients.
In spite of their limited daily calcium intake, all subjects investigated were deemed to be in calcium balance. In agreement with the latter but not with hypocalcemia, the urinary excretion of hydroxyproline, the plasma concentration of alkaline phosphatase (total and the bone isoenzyme), and tartrate-resistant acid phosphatase (markers of bone turnover, osteoblast activity and osteoclast function, respectively) were found to be within normal values. The latter strongly suggests normal parathyroid status.
As observed by other investigators (16) a significant, positive relationship (r = 0.503, p < 0.05) could be established between calcemia as a function of albuminemia (Fig. 1A). Data from LL patients, however, showed no significant trend (r = 0.031, p > 0.05) (Fig. 1B).
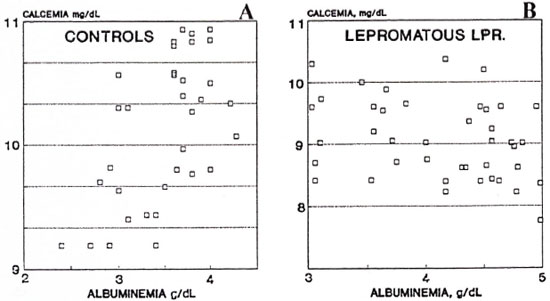
Fig. 1. A -Relationship between plasma calcium and albumin concentrations in the plasma of 36 contacts (r = 0.503, p < 0.05). B = Relationship between plasma calcium and albumin concentrations in the plasma of 34 LL patients (r = 0.031, p > 0.05).
Since the overall information obtained suggested an abnormal relationship between calcium and serum proteins, an experiment was devised to assess the competition between [Ca+ + ] and [H+] toward the protein binding of the former (Fig. 2).
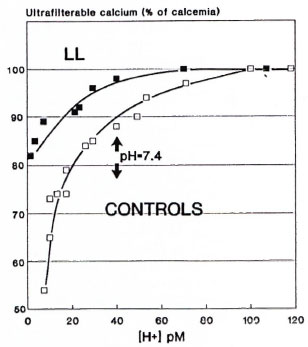
Fig. 2. Relationship between ultrafilterable plasma calcium (expressed as percentage of total calcium) and hydrogen ion concentrations of plasma pools of LL patients and their contacts (see text for further details).
At normal pH values, the plasma proteins of LL patients bound a smaller proportion of total calcium than did the plasma proteins of the contacts. The LL patients are thus in equilibrium with a normal concentration of ionized calcium in their plasma.
DISCUSSION
In analyzing the potential causes leading to hypocalcemia, and in agreement with Rao and Saha (21), undernutrition does not appear as a likely explanation because of the fact that the intake of nutrients by the LL patients were quite close to some dietary goals (22).
Similarly, osteomalacia was discarded as a plausible cause for LL hypocalcemia because of the normal plasma levels of 1,25-dihydroxyvitamin D3 and normal calcium absorption. Bone lesions in leprosy characteristically are resorptive in nature (15) and, therefore, hyper-and not hypocalcemia would have been expected. When investigating the osteoclastic resorption in maxillary alveolar bone in LL patients, Marks and Sabramaniam (11) observed the presence of large numbers of Mycobacterium leprae close to osteoclastic lesions, and they advanced the hypothesis of accelerated bone resorption by the release of some product from the neighboring bacteria. A number of studies have been reported in which hypocalcemia was demonstrated associated with both low (8,9) as well as high (1 and our study) plasma protein levels. The size of the plasma protein compartment then cannot be invoked to explain the hypocalcemia of LL patients.
Rao and Saha (21) have suggested impaired end-organ responsiveness to parathyroid hormone or increased levels of calcitonin as likely causes of LL hypocalcemia. The findings reported in this paper do not support these hypotheses.
The overall information afforded by our present data indicates that the hypocalcemia of LL patients is the consequence of the altered ability of plasma proteins to bind calcium. Quantitative Ca-binding experiments with purified plasma proteins are currently in progress in our laboratory to gain further insight into the equilibrium [Ca-Proteinate  [Ca++ ] + [proteinsn-] in the plasma of LL patients that leads to a normal concentration of ionized calcium and, in turn, a normal parathyroid status as indicated by several markers.
[Ca++ ] + [proteinsn-] in the plasma of LL patients that leads to a normal concentration of ionized calcium and, in turn, a normal parathyroid status as indicated by several markers.
Acknowledgment. A grant from the Consejo Nacional de Investigaciones Científicas y Técnicas partially supported this work. Dra. Adriana S. Dusso (Washington University, St. Louis, Missouri U.S.A.) kindly measured the plasma levels of 1,25-dihydroxy vitamin D3.
REFERENCES
1. BAJI, P. S., KHER, J. R., GANERIWAL, S. K., REDDY, B. V. and BULAKH P. M. Electrophoretic pattern of proteins in lepromatous leprosy. Lepr. India 54(1982)82-93.
2. CHEN, J., YAM, L. T., JANCKILA, A. J., Li, C. and LAM, W. K. W. Significance of "high" acid phosphatase activity in the serum of normal children. Clin. Chem. 25(1979)719-721.
3. CLARK, L. C. and THOMPSON, H. L Determination of creatinine. Anal. Chem. 21(1949)1218-1220.
4. DHOPLE, A. M. and MASAR, N. G. Studies in the blood chemistry of leprosy. Lepr. India 34(1962)299-305.
5. DOUMAS, B. T. and BIGGS, H. G. Determination of serum albumin. Stand. Meth. Clin. Chem. 7(1972)175-188.
6. DUSSO, A. S., FINCH, J., BROWN, A., RITTER, C, DELMEZ, J., SCHREINER, G. and SLATOPOLSKY, E. Extrarenal production of calcitriol in normal and uremic humans. J. Clin. Endocrinol. Metab. 72(1991)157-164.
7. GORNAL, A., BARDAWILL, C. and DAVID, M. Determination of serum proteins by means ofa biuret reaction. J. Biol. Chem. 177(1949)751-754.
8. KARAT, A. B. A. and RAO, P. S. S. Hacmatological profile in leprosy. II. Relationship to severity of disease and treatment status. Lepr. India 50(1978)18-25.
9. KUMAR, B., SEHGAL, S., GANGULY, N. K., KAUR, S. and CHAKRAVARTI, R. N. Total and differential scrum proteins and globulins in leprosy. Lepr. India 54(1982)263-269.
10. KUMAR, N., MALHOTRA, V., SINGH, R., VIJ, J. C. and ANAND, B. S. Structure and function of the small bowel in lepromatous leprosy. Int. J. Lepr. 50(1982)148-151.
11. MARKS, S. C, JR. and SUHRAMANIAM, K. The cellular basis for alveolar bone loss in leprosy. Lepr. Rev. 49(1978)297-303.
12. NIGAM, P., MUKHIJA, R. D., AGRAWAL, A. K., SATI, T. R. and KAPOOR, K. K. Serum cations (calcium and magnesium) in leprosy. Indian J. Lepr. 57(1985)529-533.
13. NOBBS, B. T., WALKER, A. W. and DAVIES, J. J. A simplified method for the estimation of urinary total hydroxyproline. Clin. Chim. Acta 64(1975)219-225.
14. PAL, R., PAL, B. and GHOSH, S. Concentration of serum calcium in leprosy. Lepr. India 55(1983)76-79.
15. PATERSON, D. E. Bone changes in leprosy; their incidence, progress, prevention and arrest. Int. J. Lepr. 29(1961)393-422.
16. PAYNE, R. B., LITTLE, A. J., WILLIAMS, R. B. and MILNER, J. R. Interpretation of serum calcium in patients with abnormal serum proteins. Br. Med. J. 4(1973)643-646.
17. PEDERSEN, K. O. Determination of calcium fractions of serum. II. Investigation of calcium ion activity and stability of important calcium complexes by an improved semimicro method. Scand. J. Clin. Lab. Invest. 25(1970)199-222.
18. PUCHE, R. C, CAFERRA, D. A. and ROSILLO, I. Bone isoenzyme of serum alkaline phosphatase measured with wheat-germ agglutinin. Clin. Chem. 34(1988)1372-1374.
19. PUCHE, R. C, RIGALLI, A., BOCANERA, R., TOZZINI, R., POUDES, G. and ROBERTI, A. A clinical test for calcium absorption in climacteric women. Medicina (Buenos Aires) 50(1990)16-20.
20. RAO, K. N., GUPTA, J. D., SEHGAL, V. N., CHAK-RABARTI, A. K. and SAHA, K. Trace elements in the sera of leprosy spectrum. Indian J. Lepr. 57(1985)556-561.
21. RAO, K. N. and SAHA, K. Undernutrition in lepromatous leprosy. II. Altered levels of serum elements; their association with the disease and not with food deprivation. Lepr. Rev. 57(1986)311-316.
22. SELECTED COMMITTEE ON NUTRITION AND HUMAN NEEDS, UNITED STATES SENATE. Dietary Goals for the United States. 2nd. edn. Washington, D.C.: U.S. Government Printing Office, 1977.
23. SINHA, S. N., GUPTA, S. C. and BISHT, D. Serum calcium and magnesium in different types of leprosy. Lepr. India 50(1978)54-56.
24. SNEDECOR, G. W. and COCIIRAN, W. G. Statistical Methods. 6th edn. Ames: Iowa State University Press, 1967.
25. TRUDEAU, A. and FREIER, E. F. Determination of calcium in urine and serum by atomic absorption stectrophotometry. Clin. Chem. 13(1967)101-105.
1. M.S., Ph.D., Investigator; Laboratório de Biologia Osea, Facultad de Medicina, Sante Fe 3100, 2000 Rosario, Argentina.
2. M.S.. Ph.D., Director, Laboratório de Biologia Osea, Facultad de Medicina, Sante Fe 3100, 2000 Rosario, Argentina.
3. M.D., Ph.D., Investigator, Division Inmunologia; Hospital Provincial de Rosario, Rosario, Argentina.
4. M.D., Servicio de Dermatologia, Hospital Provincial de Rosario, Rosario, Argentina.
Reprint requests to Dr. Puche.
Received for publication on 20 April 1993.
Accepted for publication on 24 May 1993.